Neonatal Hypoxic-ischemic Encephalopathy: A Radiological Review
- PMID: 28553370
- PMCID: PMC5437770
- DOI: 10.4103/1817-1745.205646
Neonatal Hypoxic-ischemic Encephalopathy: A Radiological Review
Abstract
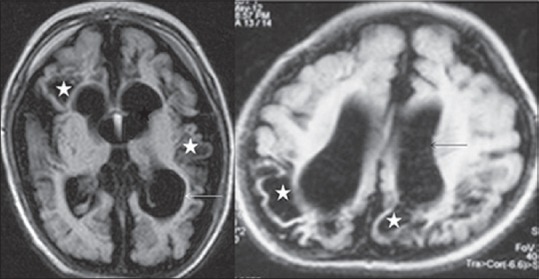
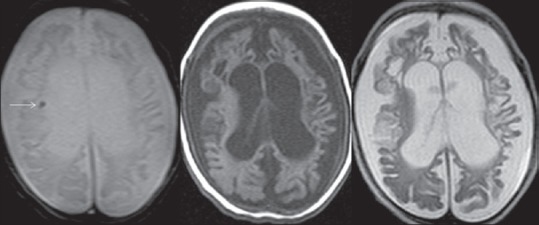
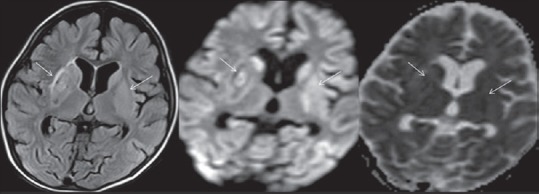
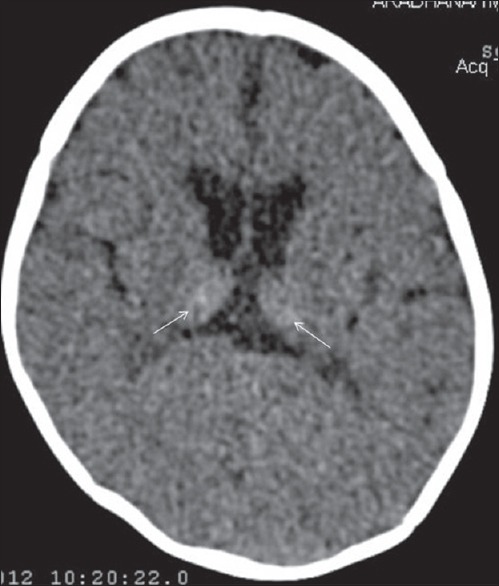
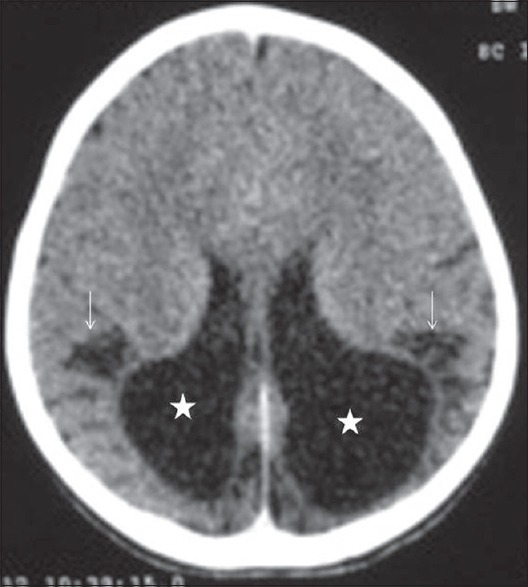
Neonatal hypoxic-ischemic encephalopathy (HIE) is a devastating condition that may result in death or severe neurologic deficits in children. Neuroimaging with cranial ultrasound (US), computed tomography and magnetic resonance imaging are valuable tools in the workup of patients with HIE. The pattern of brain injury depends on the severity and duration of hypoxia and degree of brain maturation. Mild to moderate HI injury results in periventricular leukomalacia and germinal matrix bleed in preterm neonates, and parasagittal watershed infarcts in full-term neonates. Severe HI injury involves deep gray matter in both term and preterm infants. Treatment of HIE is largely supportive. The current article reviews the etiopathophysiology and clinical manifestations of HIE, role of imaging in the evaluation of the condition, patterns of brain injury in term and preterm neonates, the treatment and the prognosis.
Keywords: Computed tomography; cranial ultrasound; hypoxic ischemic encephalopathy; magnetic resonance imaging.
Conflict of interest statement
There are no conflicts of interest.
Figures








References
-
- Kurinczuk JJ, White-Koning M, Badawi N. Epidemiology of neonatal encephalopathy and hypoxic-ischaemic encephalopathy. Early Hum Dev. 2010;86:329–38. - PubMed
-
- Barkovich AJ, editor. Pediatric Neuroimaging. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2005. Brain and spine injuries in infancy and childhood; pp. 190–290.
-
- Zarifi MK, Astrakas LG, Poussaint TY, Plessis Ad A, Zurakowski D, Tzika AA. Prediction of adverse outcome with cerebral lactate level and apparent diffusion coefficient in infants with perinatal asphyxia. Radiology. 2002;225:859–70. - PubMed
-
- Ferriero DM. Neonatal brain injury. N Engl J Med. 2004;351:1985–95. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources