

Irreducible Anterior Shoulder Dislocation with Interposition of the Long Head of the Biceps and Greater Tuberosity Fracture: A Case Report and Review of the Literature
- PMID: 28553421
- PMCID: PMC5427706
- DOI: 10.2174/1874325001711010327
Irreducible Anterior Shoulder Dislocation with Interposition of the Long Head of the Biceps and Greater Tuberosity Fracture: A Case Report and Review of the Literature
Abstract
Background: Failure of closed manipulative reduction of an acute anterior shoulder dislocation is seldom reported in the literature and is usually due to structural blocks such as soft tissue entrapment (biceps, subscapularis, labrum), bony fragments (glenoid, greater tuberosity) and severe head impaction (Hill-Sachs lesion).
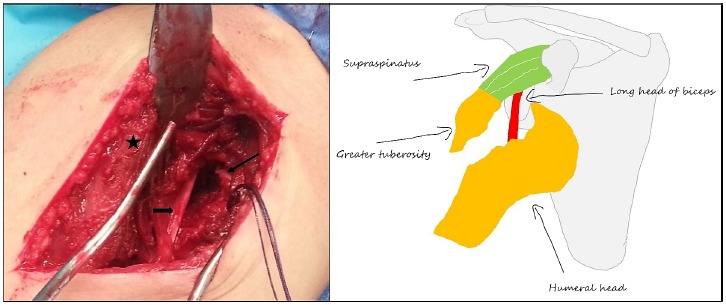
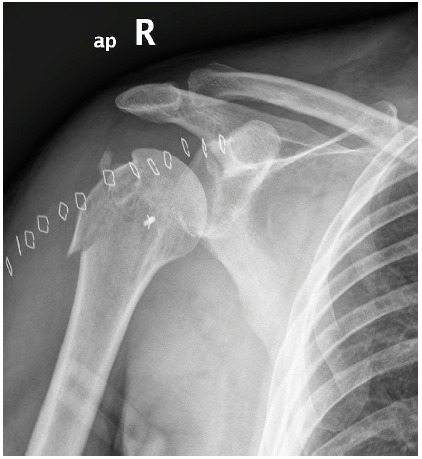
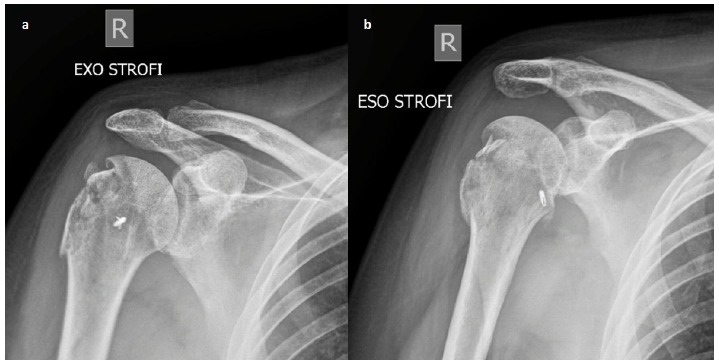
Case report: We present a case of an irreducible anterior shoulder dislocation in a 57-year-old male patient after a road-traffic accident. He had severe impaction of the head underneath glenoid rim and associated fracture of the greater tuberosity. Closed reduction performed in the emergency room under sedation and later at the theatre under general anaesthesia was unsuccessful. Open reduction using the dectopectoral approach revealed that the reason for obstruction was the posterolateral entrapment of the biceps tendon between the humeral head and the tuberosity fragment. Reduction was achieved after subscapularis tenotomy and opening of the joint; the tuberosity fragment was fixed with transosseous sutures and the long head of the biceps tendon was tenodesized. The patient had an uneventful postoperative recovery and at his last follow up, 12 months postoperatively, he had a stable joint, full range of motion and a Constant score of 90.
Conclusion: A comprehensive literature review revealed 22 similar reports affecting a total of 30 patients. Interposition of the LHBT alone or in combination with greater tuberosity fracture was the most common obstacle to reduction, followed by subscapularis tendon interposition and other less common reasons. Early surgical intervention with open reduction and confrontation of associated injuries is mandatory for a successful outcome.
Keywords: Anterior; Greater tuberosity fracture; Irreducible; Long head of biceps; Open reduction; Shoulder dislocation.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources