

Use of Chlorothiazide in the Management of Central Diabetes Insipidus in Early Infancy
- PMID: 28553553
- PMCID: PMC5434263
- DOI: 10.1155/2017/2407028
Use of Chlorothiazide in the Management of Central Diabetes Insipidus in Early Infancy
Abstract
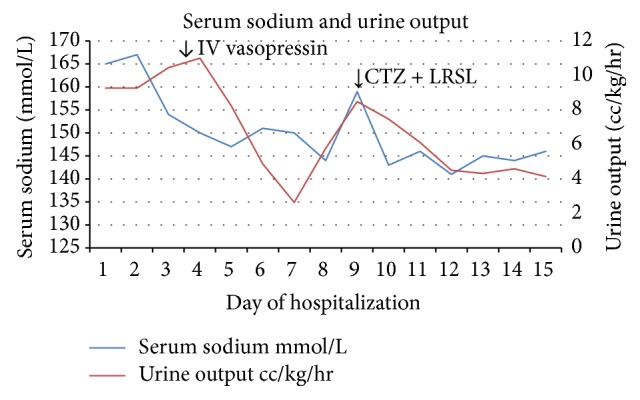
Management of central diabetes insipidus in infancy is challenging. The various forms of desmopressin, oral, subcutaneous, and intranasal, have variability in the duration of action. Infants consume most of their calories as liquids which with desmopressin puts them at risk for hyponatremia and seizures. There are few cases reporting chlorothiazide as a temporizing measure for central diabetes insipidus in infancy. A male infant presented on day of life 30 with holoprosencephaly, cleft lip and palate, and poor weight gain to endocrine clinic. Biochemical tests and urine output were consistent with central diabetes insipidus. The patient required approximately 2.5 times the normal fluid intake to keep up with the urine output. Patient was started on low renal solute load formula and oral chlorothiazide. There were normalization of serum sodium, decrease in fluid intake close to 1.3 times the normal, and improved urine output. There were no episodes of hyponatremia/hypernatremia inpatient. The patient had 2 episodes of hypernatremia in the first year of life resolving with few hours of hydration. Oral chlorothiazide is a potential bridging agent for treatment of central DI along with low renal solute load formula in early infancy. It can help achieve adequate control of DI without wide serum sodium fluctuations.
Figures
References
-
- Brandle M., Vernazza P. L., Oesterle M., Galeazzi R. L. Cerebral toxoplasmosis with central diabetes insipidus and panhypopituitarism in a patient with AIDS. Schweizerische Medizinische Wochenschrift. 1995;125(14):684–687. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
