

What We Have Learned and What We Have Missed in Tuberculosis Pathophysiology for a New Vaccine Design: Searching for the "Pink Swan"
- PMID: 28555137
- PMCID: PMC5430026
- DOI: 10.3389/fimmu.2017.00556
What We Have Learned and What We Have Missed in Tuberculosis Pathophysiology for a New Vaccine Design: Searching for the "Pink Swan"
Abstract
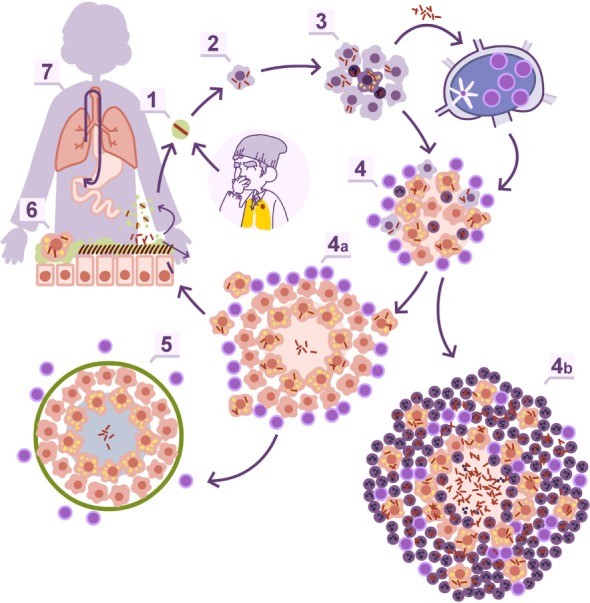
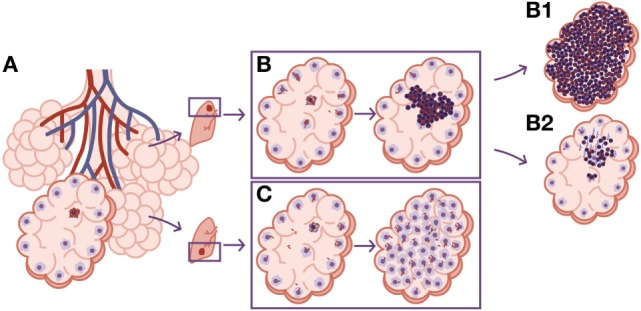
This is a call to encourage the search for a new vaccine to stop the progression of Mycobacterium tuberculosis infection to tuberculosis (TB) disease. TB is a highly discreet and stigmatized disease, with a massive impact on human health. It has killed 1.2 billion people in the last 200 years and still kills 1.5 million people per year. Over the last 20 years, the TB vaccine field has experienced spectacular developments, and we have learned about (1) the importance of the Th1 response in controlling infection, mainly against RD1 and Ag85 antigens; (2) the stability of the antigenic repertoire; (3) the dynamics of M. tuberculosis granulomas; or (4) the link between typical and atypical pulmonary TB and the immune status of the host. However, we still do not (1) know how to avoid M. tuberculosis infection and reinfection; (2) understand the major role of the increase in lesion size in progression from infection to disease; (3) the role of interlobular septa in encapsulating pulmonary lesions; or (4) the role of neutrophilic infiltration and an exaggerated inflammatory response in the development of TB disease. These are strong reasons to pursue new, imaginative proposals involving both the antibody response and a balanced, tolerant immune response that averts progression toward TB. So far, the scientific mindset has been quite monolithic and has mainly focused on the stimulation of conventional T cells. But this approach has failed. For that reason, we are seeking unconventional perspectives to find a "pink swan," a more efficacious and safer vaccine candidate.
Keywords: Mycobacterium tuberculosis; Mycobacterium tuberculosis tolerance; bacillus Calmette–Guerin vaccine; damage theory; dynamic hypothesis; pink swan.
Figures





References
-
- Platt AE. Why don’ we stop tuberculosis? World Watch (1994) 7(4):31–4. - PubMed
-
- Sagili KD, Satyanarayana S, Chadha SS. Is knowledge regarding tuberculosis associated with stigmatising and discriminating attitudes of general population towards tuberculosis patients? Findings from a community based survey in 30 districts of India. PLoS One (2016) 11(2):e0147274.10.1371/journal.pone.0147274 - DOI - PMC - PubMed
-
- Sutherland I. The evolution of clinical tuberculosis in adolescents. Tubercle (1966) 47(3):308.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous