

Antenatal management of fetal neurosurgical diseases
- PMID: 28555310
- PMCID: PMC5496971
- DOI: 10.1007/s00381-017-3442-x
Antenatal management of fetal neurosurgical diseases
Abstract
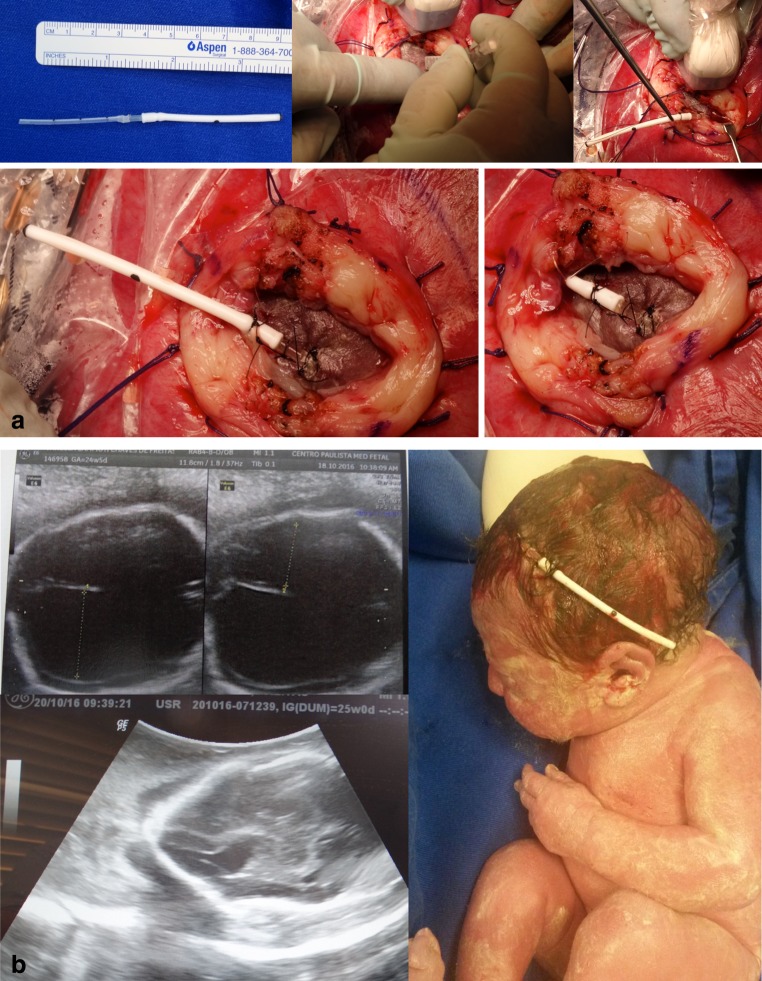
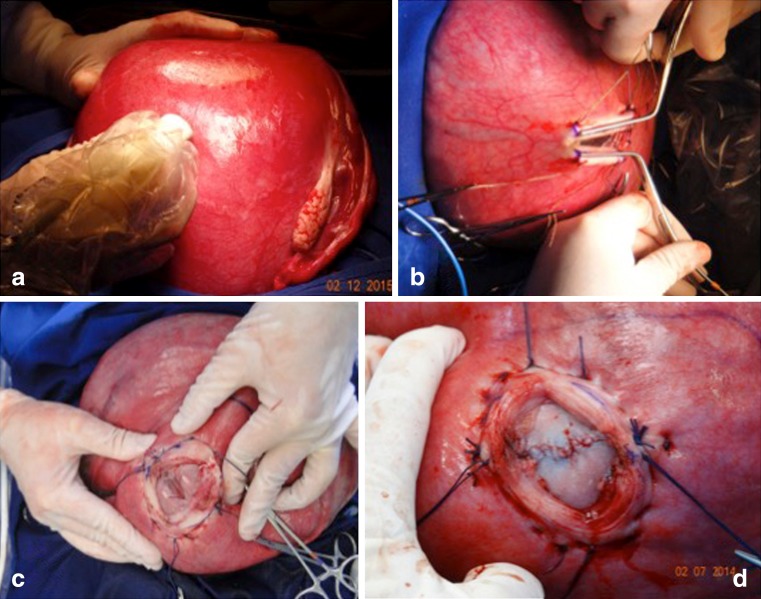
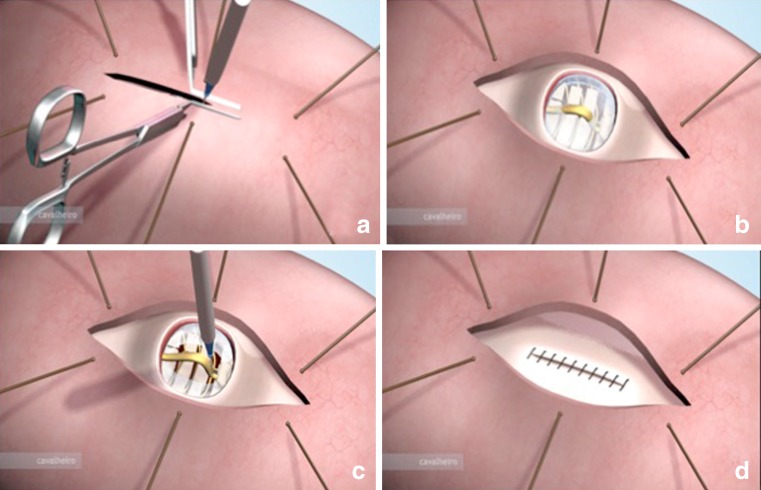
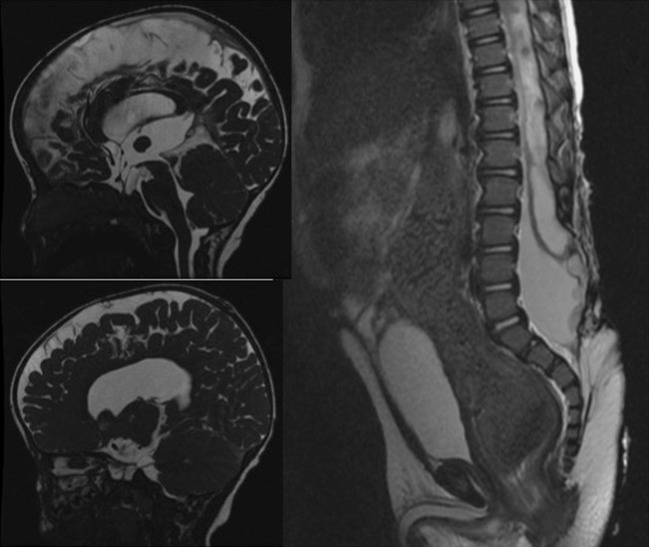
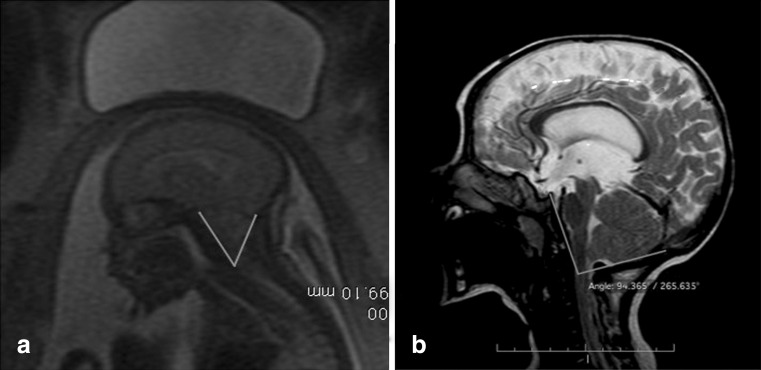
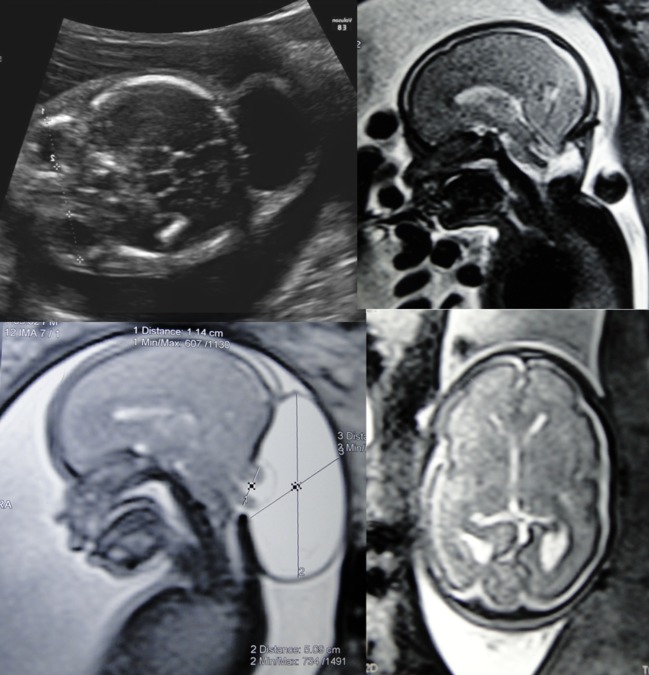
The advance in the imaging tools during the pregnancy (ultrasound and magnetic resonance) allowed the early diagnose of many fetal diseases, including the neurological conditions. This progress brought the neurosurgeons the possibility to propose treatments even before birth. Myelomeningocele is the most recognized disease that can be treated during pregnancy with a high rate of success. Additionally, this field can be extended to other conditions such as hydrocephalus and encephaloceles. However, each one of these diseases has nuances in the diagnostic evaluation that should fit the requirements to perform the fetal procedure and overbalance the benefits to the patients. In this article, the authors aim to review the neurosurgical aspects of the antenatal management of neurosurgical conditions based on the experience of a pediatric neurosurgery center.
Keywords: Cephalocentesis; Encephalocele; Hydrocephalus; Myelomeningocele; Ventricle-amniotic shunt.
Conflict of interest statement
None.
Figures




References
-
- Charpentier A (1987) Hydrocephalus. In: Grandin EH, Charpentier A (eds) Cyclopedia of obstetrics and gynecology. W. Wood & Company, New York, p 262
-
- Barke MW, Scarbough JI, O’Gorman L, Thompson WB., Jr Intrauterine ventriculography of the hydrocephalic fetus. Obstet Gynecol. 1966;28:568–570. - PubMed
-
- Kellner KR, Cruz AC, Gelman SR, Vries JK, Spellacy WN. Percutaneous fetal ventriculography: a simplified technique to aid in management of the hydrocephalic fetus. J Reprod Med. 1980;24:225–228. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
