

Accuracy of Capillary and Arterial Whole Blood Glucose Measurements Using a Glucose Meter in Patients under General Anesthesia in the Operating Room
- PMID: 28557817
- PMCID: PMC5561475
- DOI: 10.1097/ALN.0000000000001708
Accuracy of Capillary and Arterial Whole Blood Glucose Measurements Using a Glucose Meter in Patients under General Anesthesia in the Operating Room
Abstract
Background: The aim of this study was to evaluate the use of a glucose meter with surgical patients under general anesthesia in the operating room.
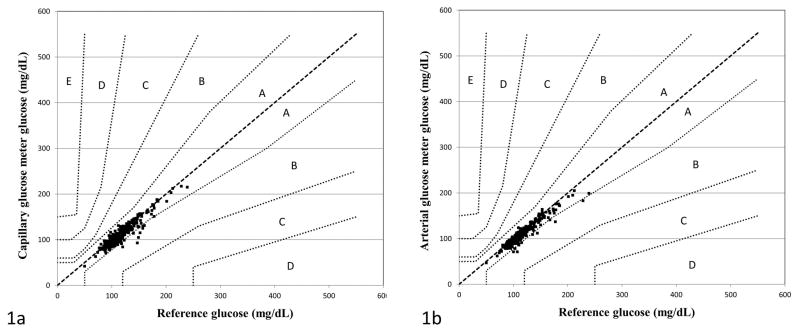
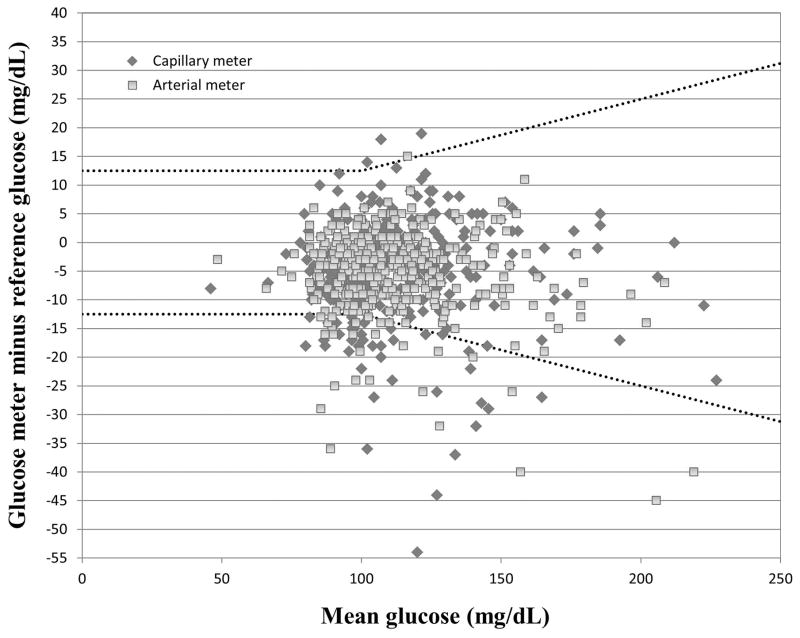
Methods: Glucose measurements were performed intraoperatively on 368 paired capillary and arterial whole blood samples using a Nova StatStrip (Nova Biomedical, USA) glucose meter and compared with 368 reference arterial whole blood glucose measurements by blood gas analyzer in 196 patients. Primary outcomes were median bias (meter minus reference), percentage of glucose meter samples meeting accuracy criteria for subcutaneous insulin dosing as defined by Parkes error grid analysis for type 1 diabetes mellitus, and accuracy criteria for intravenous insulin infusion as defined by Clinical and Laboratory Standards Institute guidelines. Time under anesthesia, patient position, diabetes status, and other variables were studied to determine whether any affected glucose meter bias.
Results: Median bias (interquartile range) was -4 mg/dl (-9 to 0 mg/dl), which did not differ from median arterial meter bias of -5 mg/dl (-9 to -1 mg/dl; P = 0.32). All of the capillary and arterial glucose meter values met acceptability criteria for subcutaneous insulin dosing, whereas only 89% (327 of 368) of capillary and 93% (344 of 368) arterial glucose meter values met accuracy criteria for intravenous insulin infusion. Time, patient position, and diabetes status were not associated with meter bias.
Conclusions: Capillary and arterial blood glucose measured using the glucose meter are acceptable for intraoperative subcutaneous insulin dosing. Whole blood glucose on the meter did not meet accuracy guidelines established specifically for more intensive (e.g., intravenous insulin) glycemic control in the acute care environment.
Conflict of interest statement
Figures
Comment in
-
Assessing Glucose Meter Accuracy: The Details Matter!Anesthesiology. 2018 May;128(5):1044-1045. doi: 10.1097/ALN.0000000000002149. Anesthesiology. 2018. PMID: 29664784 No abstract available.
-
In Reply.Anesthesiology. 2018 May;128(5):1045-1046. doi: 10.1097/ALN.0000000000002150. Anesthesiology. 2018. PMID: 29664785 No abstract available.
References
-
- Centers for Disease Control and Prevention. [Accessed December 17, 2015];2014 National Diabetes Statistics Report. http://www.cdc.gov/diabetes/data/statistics/2014statisticsreport.html.
-
- NICE-SUGAR Study Investigators. Intensive versus conventional glucose control in critically ill patients. N Engl J Med. 2009;360:1283–1297. - PubMed
-
- Lewis K, Kane-Gill S, Bobek M, Dasta J. Intensive insulin therapy in critically ill patients. Ann Pharmacother. 2004;38:1243–51. - PubMed
-
- Van den Berghe G, Wouters P, Weekers F, Verwaest C, Bruyninckx F, Schietz M, Vlasselaers D, Ferdinande P, Lauwers P, Bouillon R. Intensive insulin therapy in critically ill patients. N Engl J Med. 2001;345:1359–67. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
