

Association between expansion of primary healthcare and racial inequalities in mortality amenable to primary care in Brazil: A national longitudinal analysis
- PMID: 28557989
- PMCID: PMC5448733
- DOI: 10.1371/journal.pmed.1002306
Association between expansion of primary healthcare and racial inequalities in mortality amenable to primary care in Brazil: A national longitudinal analysis
Abstract
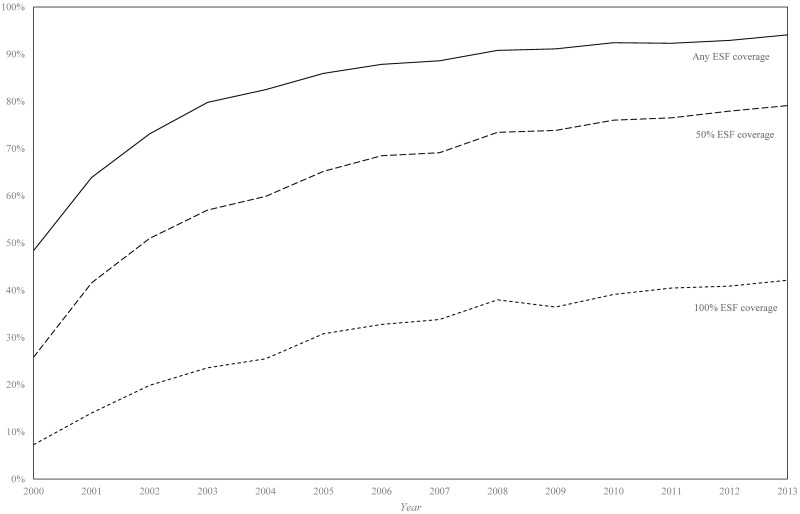
Background: Universal health coverage (UHC) can play an important role in achieving Sustainable Development Goal (SDG) 10, which addresses reducing inequalities, but little supporting evidence is available from low- and middle-income countries. Brazil's Estratégia de Saúde da Família (ESF) (family health strategy) is a community-based primary healthcare (PHC) programme that has been expanding since the 1990s and is the main platform for delivering UHC in the country. We evaluated whether expansion of the ESF was associated with differential reductions in mortality amenable to PHC between racial groups.
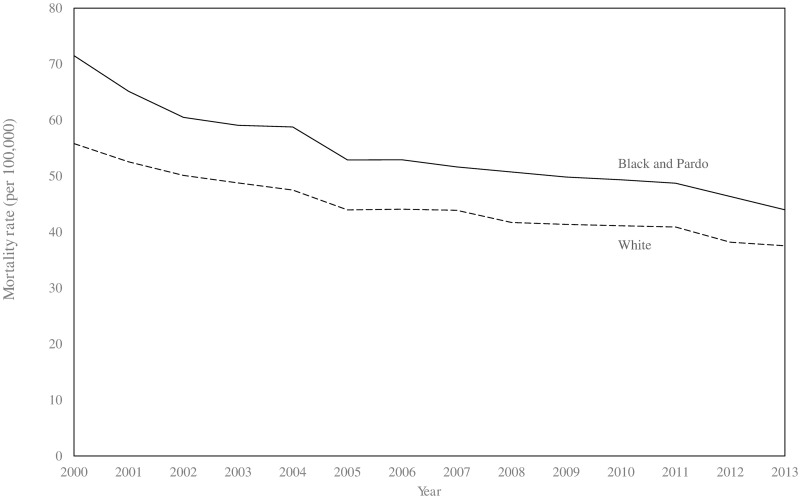
Methods and findings: Municipality-level longitudinal fixed-effects panel regressions were used to examine associations between ESF coverage and mortality from ambulatory-care-sensitive conditions (ACSCs) in black/pardo (mixed race) and white individuals over the period 2000-2013. Models were adjusted for socio-economic development and wider health system variables. Over the period 2000-2013, there were 281,877 and 318,030 ACSC deaths (after age standardisation) in the black/pardo and white groups, respectively, in the 1,622 municipalities studied. Age-standardised ACSC mortality fell from 93.3 to 57.9 per 100,000 population in the black/pardo group and from 75.7 to 49.2 per 100,000 population in the white group. ESF expansion (from 0% to 100%) was associated with a 15.4% (rate ratio [RR]: 0.846; 95% CI: 0.796-0.899) reduction in ACSC mortality in the black/pardo group compared with a 6.8% (RR: 0.932; 95% CI: 0.892-0.974) reduction in the white group (coefficients significantly different, p = 0.012). These differential benefits were driven by greater reductions in mortality from infectious diseases, nutritional deficiencies and anaemia, diabetes, and cardiovascular disease in the black/pardo group. Although the analysis is ecological, sensitivity analyses suggest that over 30% of black/pardo deaths would have to be incorrectly coded for the results to be invalid. This study is limited by the use of municipal-aggregate data, which precludes individual-level inference. Omitted variable bias, where factors associated with ESF expansion are also associated with changes in mortality rates, may have influenced our findings, although sensitivity analyses show the robustness of the findings to pre-ESF trends and the inclusion of other municipal-level factors that could be associated with coverage.
Conclusions: PHC expansion is associated with reductions in racial group inequalities in mortality in Brazil. These findings highlight the importance of investment in PHC to achieve the SDGs aimed at improving health and reducing inequalities.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Macinko J, Dourado I, Aquino R, Bonolo Pde F, Lima-Costa MF, Medina MG, et al. Major expansion of primary care in Brazil linked to decline in unnecessary hospitalization. Health Aff (Millwood). 2010;29(12):2149–60. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
