

Kidney volume measurement methods for clinical studies on autosomal dominant polycystic kidney disease
- PMID: 28558028
- PMCID: PMC5448775
- DOI: 10.1371/journal.pone.0178488
Kidney volume measurement methods for clinical studies on autosomal dominant polycystic kidney disease
Abstract
Background: In autosomal dominant polycystic kidney disease (ADPKD), total kidney volume (TKV) is regarded as an important biomarker of disease progression and different methods are available to assess kidney volume. The purpose of this study was to identify the most efficient kidney volume computation method to be used in clinical studies evaluating the effectiveness of treatments on ADPKD progression.
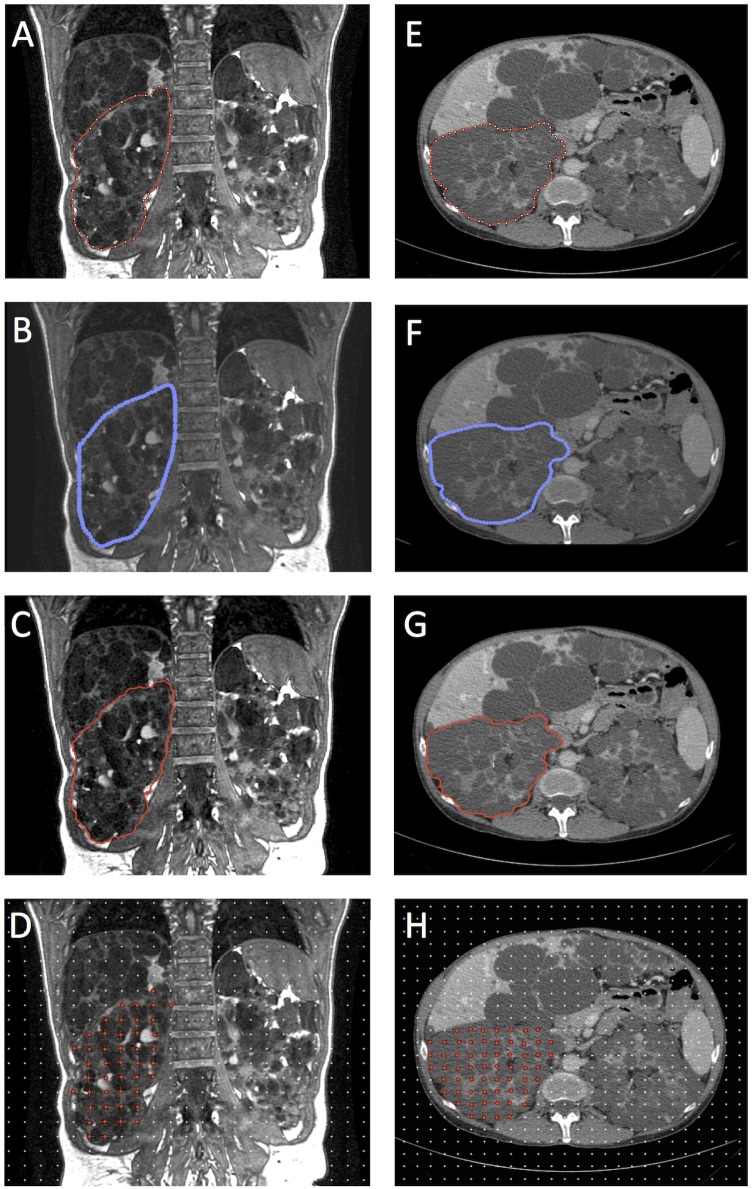
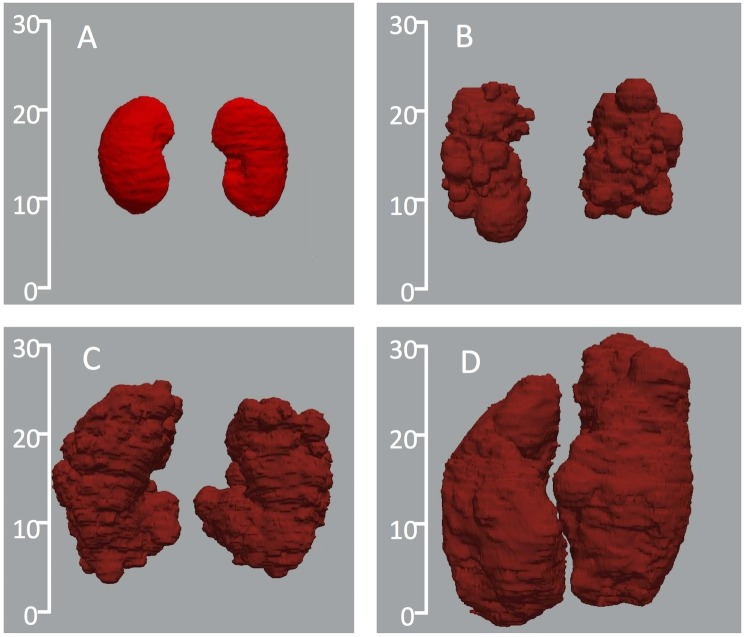
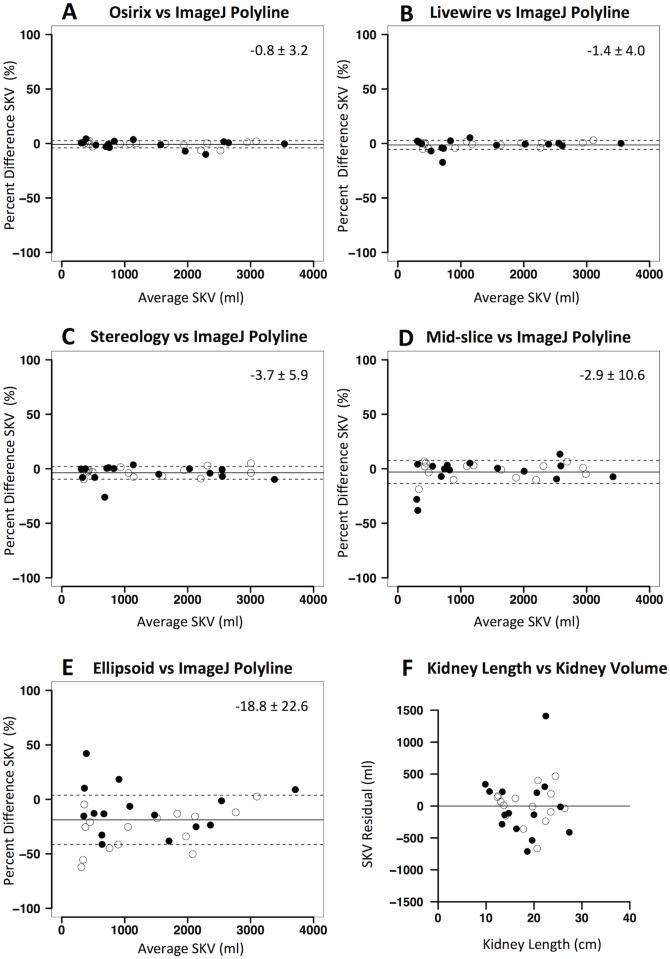
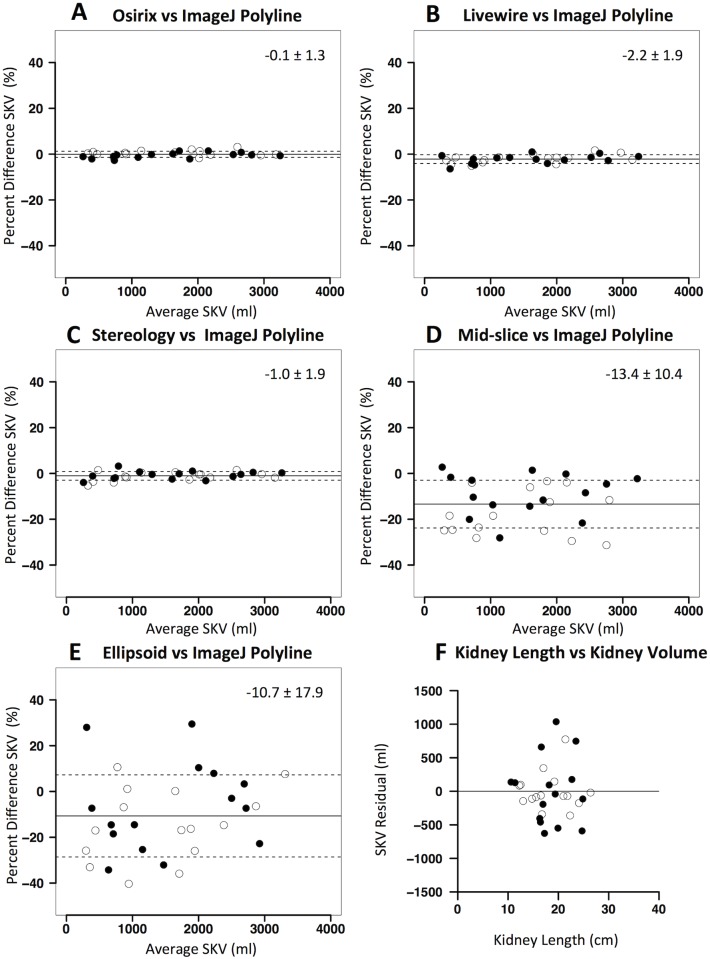
Methods and findings: We measured single kidney volume (SKV) on two series of MR and CT images from clinical studies on ADPKD (experimental dataset) by two independent operators (expert and beginner), twice, using all of the available methods: polyline manual tracing (reference method), free-hand manual tracing, semi-automatic tracing, Stereology, Mid-slice and Ellipsoid method. Additionally, the expert operator also measured the kidney length. We compared different methods for reproducibility, accuracy, precision, and time required. In addition, we performed a validation study to evaluate the sensitivity of these methods to detect the between-treatment group difference in TKV change over one year, using MR images from a previous clinical study. Reproducibility was higher on CT than MR for all methods, being highest for manual and semiautomatic contouring methods (planimetry). On MR, planimetry showed highest accuracy and precision, while on CT accuracy and precision of both planimetry and Stereology methods were comparable. Mid-slice and Ellipsoid method, as well as kidney length were fast but provided only a rough estimate of kidney volume. The results of the validation study indicated that planimetry and Stereology allow using an importantly lower number of patients to detect changes in kidney volume induced by drug treatment as compared to other methods.
Conclusions: Planimetry should be preferred over fast and simplified methods for accurately monitoring ADPKD progression and assessing drug treatment effects. Expert operators, especially on MR images, are required for performing reliable estimation of kidney volume. The use of efficient TKV quantification methods considerably reduces the number of patients to enrol in clinical investigations, making them more feasible and significant.
Conflict of interest statement
Figures
References
-
- Grantham JJ. The etiology, pathogenesis, and treatment of autosomal dominant polycystic kidney disease: recent advances. Am J Kidney Dis. 1996;28: 788–803. - PubMed
-
- Grantham JJ, Torres VE, Chapman AB, Guay-Woodford LM, Bae KT, King BF Jr, et al. ; CRISP Investigators. Volume progression in polycystic kidney disease. N Engl J Med. 2006;354: 2122–2130. - PubMed
-
- King BF, Reed JE, Bergstralh EJ, Sheedy PF 2nd, Torres VE. Quantification and longitudinal trends of kidney, renal cyst, and renal parenchyma volumes in autosomal dominant polycystic kidney disease. J Am Soc Nephrol. 2000;11: 505–1511. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
