

Calretinin as a blood-based biomarker for mesothelioma
- PMID: 28558669
- PMCID: PMC5450182
- DOI: 10.1186/s12885-017-3375-5
Calretinin as a blood-based biomarker for mesothelioma
Abstract
Background: Malignant mesothelioma (MM) is a deadly cancer mainly caused by previous exposure to asbestos. With a latency period up to 50 years the incidence of MM is still increasing, even in countries that banned asbestos. Secondary prevention has been established to provide persons at risk regular health examinations. An earlier detection with tumor markers might improve therapeutic options. Previously, we have developed a new blood-based assay for the protein marker calretinin. Aim of this study was the verification of the assay in an independent study population and comparison with the established marker mesothelin.
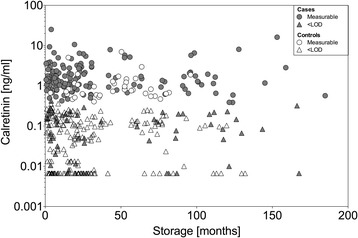
Methods: For a case-control study in men, a total of 163 cases of pleural MM and 163 controls were available from Australia, another 36 cases and 72 controls were recruited in Germany. All controls had asbestosis and/or plaques. Calretinin and mesothelin were determined by ELISA (enzyme-linked immunosorbent assay) in serum or plasma collected prior to therapy. We estimated the performance of both markers and tested factors potentially influencing marker concentrations like age, sample storage time, and MM subtype.
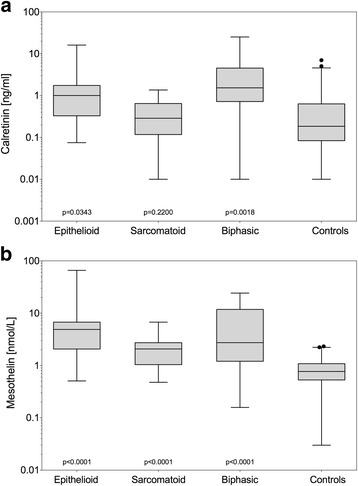
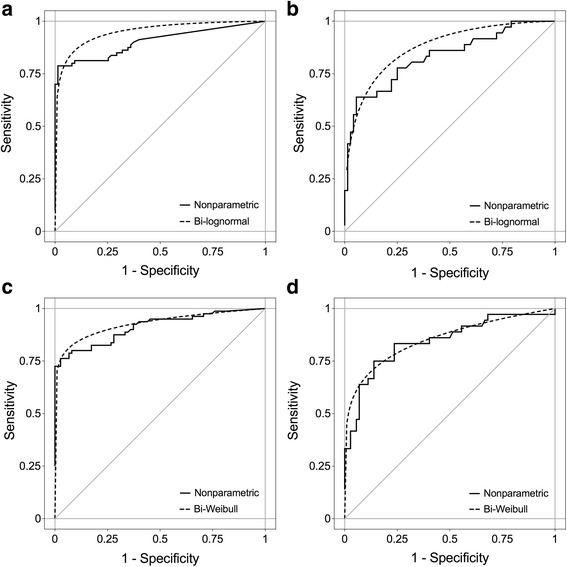
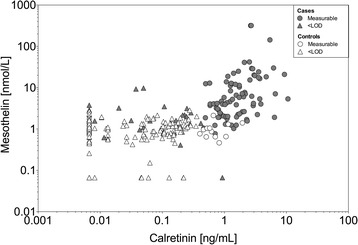
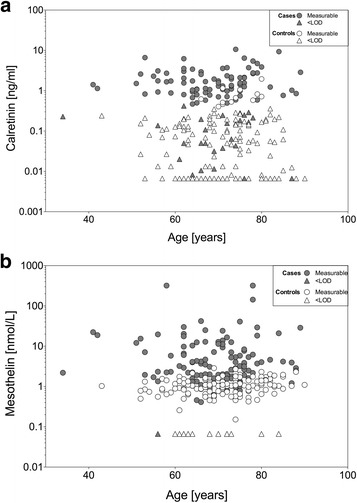
Results: Calretinin was able to detect all major subtypes except for sarcomatoid MM. Calretinin showed a similar performance in Australian and German men. At a pre-defined specificity of 95% the sensitivity of calretinin reached 71% and that of mesothelin 69%, when excluding sarcomatoid MM. At 97% specificity, the combination with calretinin increased the sensitivity of mesothelin from 66% to 75%. Sample storage time did not influence the results. In controls the concentrations of calretinin increased 1.87-fold (95% CI 1.10-3.20) per 10 years of age and slightly more for mesothelin (2.28, 95% CI 1.30-4.00).
Conclusions: Calretinin could be verified as a blood-based marker for MM. The assay is robust and shows a performance that is comparable to that of mesothelin. Retrospective analyses would not be limited by storage time. The high specificity supports a combination of calretinin with other markers. Calretinin is specific for epithelioid and biphasic MM but not the rarer sarcomatoid form. Molecular markers like calretinin and mesothelin are promising tools to improve and supplement the diagnosis of MM and warrant further validation in a prospective study.
Keywords: Asbestos; Biomarker panel; Biphasic; Calretinin; Early diagnosis; Epithelioid; Mesothelin; Mesothelioma; Plasma; Sarcomatoid; Serum.
Figures


References
-
- IARC. IARC monographs on the evaluation of the carcinogenic risk of chemicals to man: asbestos. IARC Monogr Eval Carcinog Risk Chem Man. 1977;14:1–106. - PubMed
-
- AMR: Australian Mesothelioma Registry 3rd annual report: Mesothelioma in Australia 2013. Canberra: Safe Work Australia; 2014.
-
- Husain AN, Colby T, Ordonez N, Krausz T, Attanoos R, Beasley MB, et al. Guidelines for pathologic diagnosis of malignant mesothelioma: 2012 update of the consensus statement from the international mesothelioma interest group. Arch Pathol Lab Med. 2013;137(5):647–667. doi: 10.5858/arpa.2012-0214-OA. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
