

Critical care at the end of life: a population-level cohort study of cost and outcomes
- PMID: 28558826
- PMCID: PMC5450109
- DOI: 10.1186/s13054-017-1711-4
Critical care at the end of life: a population-level cohort study of cost and outcomes
Abstract
Background: Despite the high cost associated with ICU use at the end of life, very little is known at a population level about the characteristics of users and their end of life experience. In this study, our goal was to characterize decedents who received intensive care near the end of life and examine their overall health care use prior to death.
Methods: This was a retrospective cohort study that examined all deaths in a 3-year period from April 2010 to March 2013 in Ontario, Canada. Using population-based health administrative databases, we examined healthcare use and cost in the last year of life.
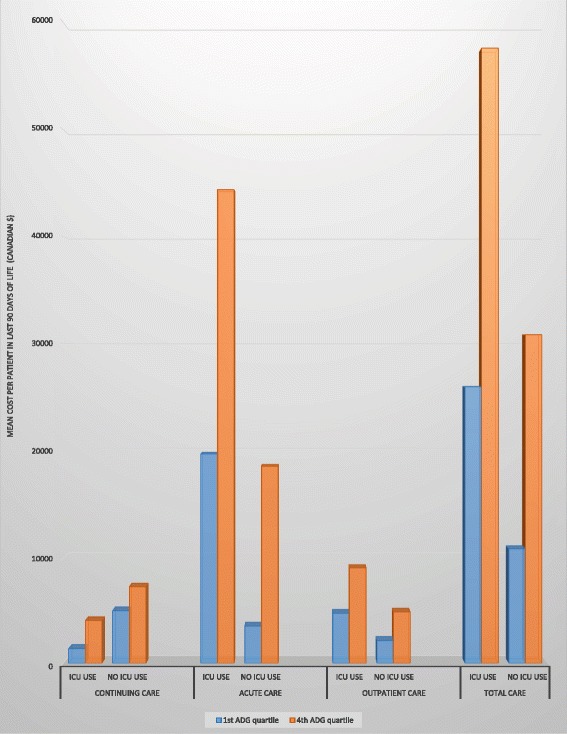
Results: There were 264,754 individuals included in the study, of whom 18% used the ICU in the last 90 days of life; 34.5% of these ICU users were older than 80 years of age and 53.0% had more than five chronic conditions. The average cost of stay for these decedents was CA$15,511 to CA$25,526 greater than for those who were not admitted to the ICU. These individuals also died more frequently in hospital (88.7% vs 36.2%), and spent more time in acute-care settings (18.7 days vs. 10.5 days).
Conclusions: We showed at a population level that a significant proportion of those with ICU use close to death are older, multi-morbid individuals who incur significantly greater costs and die largely in hospital, with higher rates of readmission, longer lengths of stay and higher rates of aggressive care.
Keywords: Costs and cost analysis; Palliative care; Terminal care.
Figures
Similar articles
-
Describing the characteristics and healthcare use of high-cost acute care users at the end of life: a pan-Canadian population-based study.BMC Health Serv Res. 2020 Oct 31;20(1):997. doi: 10.1186/s12913-020-05837-8. BMC Health Serv Res. 2020. PMID: 33129316 Free PMC article.
-
Does Primary Care Model Effect Healthcare at the End of Life? A Population-Based Retrospective Cohort Study.J Palliat Med. 2017 Apr;20(4):344-351. doi: 10.1089/jpm.2016.0283. Epub 2016 Nov 28. J Palliat Med. 2017. PMID: 27893954
-
Use of intensive care at the end of life in the United States: an epidemiologic study.Crit Care Med. 2004 Mar;32(3):638-43. doi: 10.1097/01.ccm.0000114816.62331.08. Crit Care Med. 2004. PMID: 15090940
-
End-of-Life Care Interventions: An Economic Analysis.Ont Health Technol Assess Ser. 2014 Dec 1;14(18):1-70. eCollection 2014. Ont Health Technol Assess Ser. 2014. PMID: 26339303 Free PMC article. Review.
-
Economic implications of end-of-life care in the ICU.Curr Opin Crit Care. 2014 Dec;20(6):656-61. doi: 10.1097/MCC.0000000000000147. Curr Opin Crit Care. 2014. PMID: 25222642 Free PMC article. Review.
Cited by
-
Emergency Department disposition decisions and associated mortality and costs in ICU patients with suspected infection.Crit Care. 2018 Jul 6;22(1):172. doi: 10.1186/s13054-018-2096-8. Crit Care. 2018. PMID: 29976238 Free PMC article.
-
Cost of Futile ICU Care in One Ontario Hospital.Inquiry. 2021 Jan-Dec;58:469580211028577. doi: 10.1177/00469580211028577. Inquiry. 2021. PMID: 34218711 Free PMC article.
-
Coaching doctors to improve ethical decision-making in adult hospitalized patients potentially receiving excessive treatment. The CODE stepped-wedge cluster randomized controlled trial.Intensive Care Med. 2024 Oct;50(10):1635-1646. doi: 10.1007/s00134-024-07588-0. Epub 2024 Sep 4. Intensive Care Med. 2024. PMID: 39230678 Free PMC article. Clinical Trial.
-
The cost of treatment and its related complications for men who receive surgery or radiation therapy for prostate cancer.Can Urol Assoc J. 2019 Aug;13(8):E236-E248. doi: 10.5489/cuaj.5598. Can Urol Assoc J. 2019. PMID: 30526806 Free PMC article.
-
Resource utilisation and description of patients perceived as receiving inappropriate critical care.Intensive Crit Care Nurs. 2019 Oct;54:29-33. doi: 10.1016/j.iccn.2019.06.003. Epub 2019 Jun 14. Intensive Crit Care Nurs. 2019. PMID: 31204107 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
