

The effectiveness of a de-implementation strategy to reduce low-value blood management techniques in primary hip and knee arthroplasty: a pragmatic cluster-randomized controlled trial
- PMID: 28558843
- PMCID: PMC5450044
- DOI: 10.1186/s13012-017-0601-0
The effectiveness of a de-implementation strategy to reduce low-value blood management techniques in primary hip and knee arthroplasty: a pragmatic cluster-randomized controlled trial
Abstract
Background: Perioperative autologous blood salvage and preoperative erythropoietin are not (cost) effective to reduce allogeneic transfusion in primary hip and knee arthroplasty, but are still used. This study aimed to evaluate the effectiveness of a theoretically informed multifaceted strategy to de-implement these low-value blood management techniques.
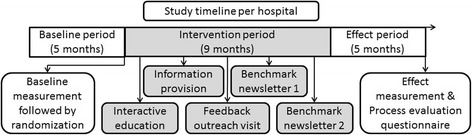
Methods: Twenty-one Dutch hospitals participated in this pragmatic cluster-randomized trial. At baseline, data were gathered for 924 patients from 10 intervention and 1040 patients from 11 control hospitals undergoing hip or knee arthroplasty. The intervention included a multifaceted de-implementation strategy which consisted of interactive education, feedback on blood management performance, and a comparison with benchmark hospitals, aimed at orthopedic surgeons and anesthesiologists. After the intervention, data were gathered for 997 patients from the intervention and 1096 patients from the control hospitals. The randomization outcome was revealed after the baseline measurement. Primary outcomes were use of blood salvage and erythropoietin. Secondary outcomes included postoperative hemoglobin, length of stay, allogeneic transfusions, and use of local infiltration analgesia (LIA) and tranexamic acid (TXA).
Results: The use of blood salvage (OR 0.08, 95% CI 0.02 to 0.30) and erythropoietin (OR 0.30, 95% CI 0.09 to 0.97) reduced significantly over time, but did not differ between intervention and control hospitals (blood salvage OR 1.74 95% CI 0.27 to 11.39, erythropoietin OR 1.33, 95% CI 0.26 to 6.84). Postoperative hemoglobin levels were significantly higher (β 0.21, 95% CI 0.08 to 0.34) and length of stay shorter (β -0.36, 95% CI -0.64 to -0.09) in hospitals receiving the multifaceted strategy, compared with control hospitals and after adjustment for baseline. Transfusions did not differ between the intervention and control hospitals (OR 1.06, 95% CI 0.63 to 1.78). Both LIA (OR 0.0, 95% CI 0.0 to 0.0) and TXA (OR 0.3, 95% CI 0.2 to 0.5) were significantly associated with the reduction in blood salvage over time.
Conclusions: Blood salvage and erythropoietin use reduced over time, but not differently between intervention and control hospitals. The reduction in blood salvage was associated with increased use of local infiltration analgesia and tranexamic acid, suggesting that de-implementation is assisted by the substitution of techniques. The reduction in blood salvage and erythropoietin did not lead to a deterioration in patient-related secondary outcomes.
Trial registration: www.trialregister.nl, NTR4044.
Keywords: De-implementation; Hip and knee arthroplasty; Low-value care; Multifaceted strategy; Perioperative autologous blood salvage; Preoperative erythropoietin.
Figures
References
-
- Smith M, Saunders R, Stuckhardt L, McGinnis JM. Best Care at Lower Cost: The Path to Continuously Learning Health Care in America. National Academies Press (US). 2013. doi:10.17226/13444. - PubMed
-
- van Bodegom-Vos L, Davidoff F, Marang-van de Mheen PJ. Implementation and de-implementation: two sides of the same coin? BMJ Qual Saf. 2016;26:495–501. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
