

Etiology and clinical presentation of birth defects: population based study
- PMID: 28559234
- PMCID: PMC5448402
- DOI: 10.1136/bmj.j2249
Etiology and clinical presentation of birth defects: population based study
Abstract
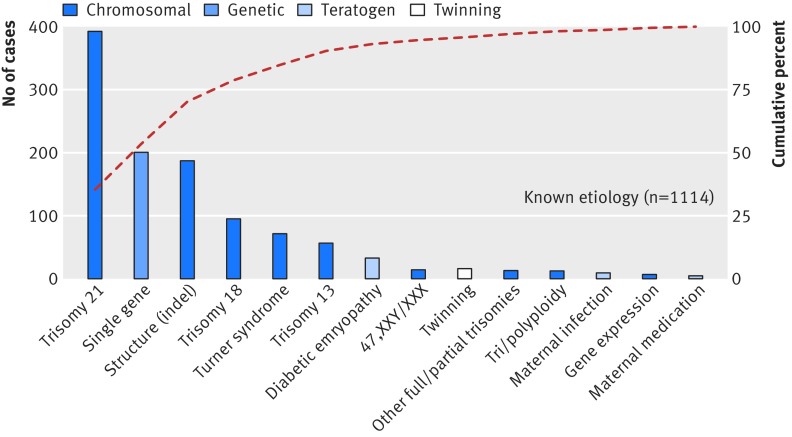
Objective To assess causation and clinical presentation of major birth defects.Design Population based case cohort.Setting Cases of birth defects in children born 2005-09 to resident women, ascertained through Utah's population based surveillance system. All records underwent clinical re-review.Participants 5504 cases among 270 878 births (prevalence 2.03%), excluding mild isolated conditions (such as muscular ventricular septal defects, distal hypospadias).Main outcome measures The primary outcomes were the proportion of birth defects with a known etiology (chromosomal, genetic, human teratogen, twinning) or unknown etiology, by morphology (isolated, multiple, minors only), and by pathogenesis (sequence, developmental field defect, or known pattern of birth defects).Results Definite cause was assigned in 20.2% (n=1114) of cases: chromosomal or genetic conditions accounted for 94.4% (n=1052), teratogens for 4.1% (n=46, mostly poorly controlled pregestational diabetes), and twinning for 1.4% (n=16, conjoined or acardiac). The 79.8% (n=4390) remaining were classified as unknown etiology; of these 88.2% (n=3874) were isolated birth defects. Family history (similarly affected first degree relative) was documented in 4.8% (n=266). In this cohort, 92.1% (5067/5504) were live born infants (isolated and non-isolated birth defects): 75.3% (4147/5504) were classified as having an isolated birth defect (unknown or known etiology).Conclusions These findings underscore the gaps in our knowledge regarding the causes of birth defects. For the causes that are known, such as smoking or diabetes, assigning causation in individual cases remains challenging. Nevertheless, the ongoing impact of these exposures on fetal development highlights the urgency and benefits of population based preventive interventions. For the causes that are still unknown, better strategies are needed. These can include greater integration of the key elements of etiology, morphology, and pathogenesis into epidemiologic studies; greater collaboration between researchers (such as developmental biologists), clinicians (such as medical geneticists), and epidemiologists; and better ways to objectively measure fetal exposures (beyond maternal self reports) and closer (prenatally) to the critical period of organogenesis.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form and declare no support from any organization for the submitted work, no financial relationships with any organizations that might have an interest in the submitted work in the previous three years, and no other relationships or activities that could appear to have influenced the submitted work.
Figures

References
-
- World Health Organization (WHO). Sixty-third World Health Assembly. Birth Defects. Report by the Secretariat. A63/10. April 2010.
-
- Centers for Disease Control and Prevention (CDC). Update on overall prevalence of major birth defects--Atlanta, Georgia, 1978-2005. MMWR Morb Mortal Wkly Rep 2008;57:1-5.pmid:18185492. - PubMed
-
- Christianson A, Howson CP, Modell B. March of Dimes Global Report on Birth Defects.The Hidden Toll of Dying and Disabled Children. March of Dimes Birth Defects Foundation, 2006.
-
- Russo CA, Elixhauser A. Hospitalizations for Birth Defects, 2004. HCUP Statistical Brief #24.U.S. Agency for Healthcare Research and Quality, 2007. - PubMed
-
- Mathews TJ, MacDorman MF, Thoma ME. Infant mortality statistics from the 2013 period linked birth/infant death data set. National vital statistics reports; National Center for Health Statistics; 2015;64(9). - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical