

Occult myeloproliferative neoplasms: not so occult any more
- PMID: 28559287
- PMCID: PMC5747619
- DOI: 10.1136/bcr-2017-219388
Occult myeloproliferative neoplasms: not so occult any more
Abstract
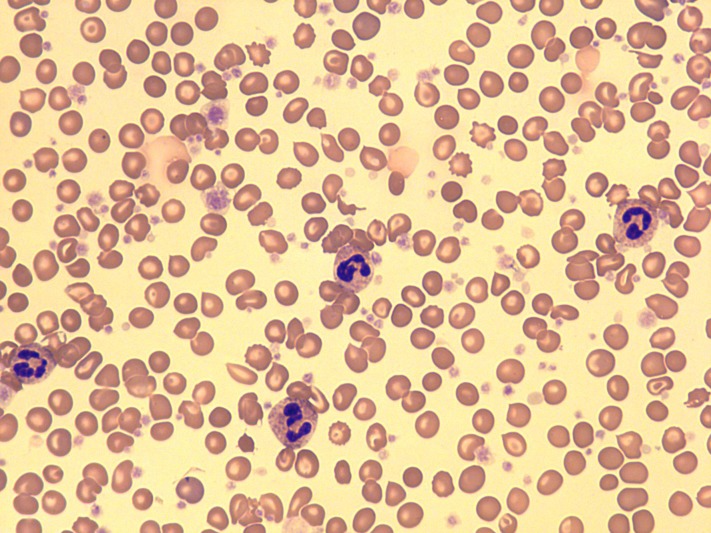
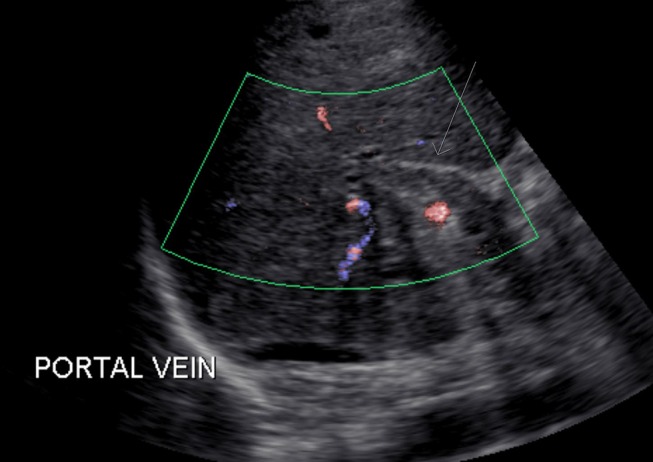
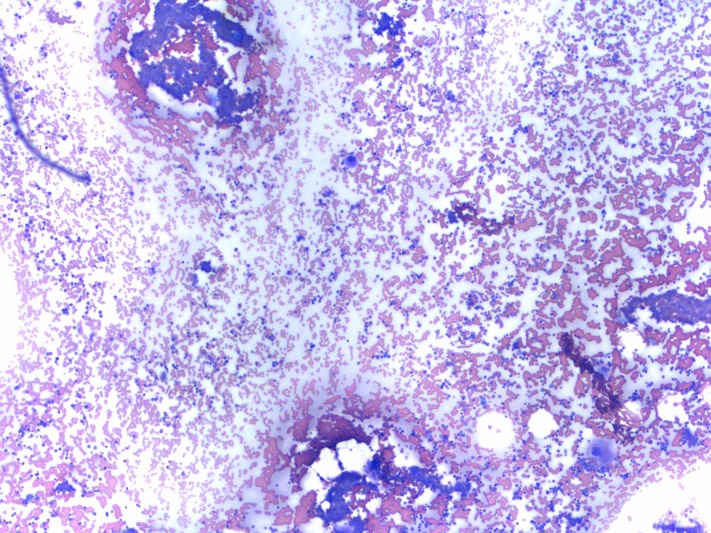
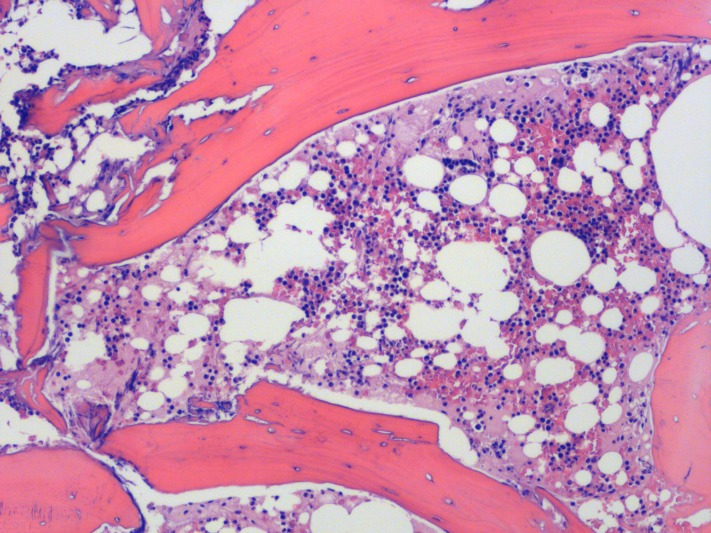
Non-cirrhotic, non-malignant portal vein thrombosis (PVT) is commonly secondary to inherited or acquired prothrombotic states. However, even after extensive workup, 25% of patients with PVT have no apparent prothrombotic aetiology identified (idiopathic PVT). Inherited conditions include factor V Leiden, PT mutation and protein C/S/AT deficiency. Acquired conditions include APS, PNH and BCR-ABL 1-negative myeloproliferative neoplasms (MPN). BCR-ABL-1 negative MPNs are the most frequent underlying prothrombotic risk factor for PVT (15%-30%). However, peripheral blood counts often remain within normal ranges in these patients with MPN because of portal hypertension sequel. Despite suggestive features of MPN in bone marrow, these patients lack adequate diagnostic criteria and are classified as occult MPN. The discovery of recurrent molecular abnormalities such as CALR gene exon 9 mutation presented a crucial advance in the diagnosis of occult MPNs. In our patient, the diagnosis of MPN was made on this basis, despite lack of peripheral evidence of MPN.
Keywords: haematology (incl blood transfusion); medical management.
© BMJ Publishing Group Ltd (unless otherwise stated in the text of the article) 2017. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Myeloproliferative neoplasms in Budd-Chiari syndrome and portal vein thrombosis: a meta-analysis.Blood. 2012 Dec 13;120(25):4921-8. doi: 10.1182/blood-2011-09-376517. Epub 2012 Oct 4. Blood. 2012. PMID: 23043069 Review.
-
Diagnostic value of the JAK2 V617F mutation for latent chronic myeloproliferative disorders in patients with Budd-Chiari syndrome and/or portal vein thrombosis.Turk J Gastroenterol. 2015 Jan;26(1):42-8. doi: 10.5152/tjg.2015.5738. Turk J Gastroenterol. 2015. PMID: 25698270
-
Next-generation sequencing in the diagnosis of non-cirrhotic splanchnic vein thrombosis.J Hepatol. 2021 Jan;74(1):89-95. doi: 10.1016/j.jhep.2020.06.045. Epub 2020 Jul 15. J Hepatol. 2021. PMID: 32679300
-
Prevalence of prothrombotic factors in patients with Budd-Chiari syndrome or non-cirrhotic nonmalignant portal vein thrombosis: A hospital-based observational study.J Gastroenterol Hepatol. 2020 Jul;35(7):1215-1222. doi: 10.1111/jgh.14925. Epub 2019 Dec 15. J Gastroenterol Hepatol. 2020. PMID: 31711259
-
Splanchnic vein thrombosis and myeloproliferative neoplasms: molecular-driven diagnosis and long-term treatment.Thromb Haemost. 2016 Jan;115(2):240-9. doi: 10.1160/TH15-04-0326. Epub 2015 Sep 3. Thromb Haemost. 2016. PMID: 26333846 Review.
Cited by
-
Detecting CALR Mutations in Splanchnic Vein Thrombosis: Who and How?J Transl Int Med. 2018 Jun 26;6(2):55-57. doi: 10.2478/jtim-2018-0015. eCollection 2018 Jun. J Transl Int Med. 2018. PMID: 29984196 Free PMC article. No abstract available.
References
-
- Valla D, Casadevall N, Huisse MG, et al. . Etiology of portal vein thrombosis in adults. A prospective evaluation of primary myeloproliferative disorders. Gastroenterology 1988;94:1063–9. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous