

doi: 10.1016/j.eats.2016.08.019.
eCollection 2016 Dec.
Basics of Elbow Arthroscopy Part I: Surface Anatomy, Portals, and Structures at Risk
Affiliations
- PMID: 28560134
- PMCID: PMC5439187
- DOI: 10.1016/j.eats.2016.08.019
Item in Clipboard
Basics of Elbow Arthroscopy Part I: Surface Anatomy, Portals, and Structures at Risk
Arthrosc Tech.
.
Abstract
As our knowledge and technology advance, the indications for elbow arthroscopy continue to grow rapidly. During this expansion, a number of new portals have been described and reported using variable nomenclature and location descriptions. Accordingly, a comprehensive review of these portals is warranted. Given the concern for potential iatrogenic injury to surrounding neurovascular structures, a discussion of these critical nerves and vessels is also timely. In this work, we review pertinent surface anatomy; portal nomenclature, locations, and utility; and review distances to the nearest structures at risk.
Figures
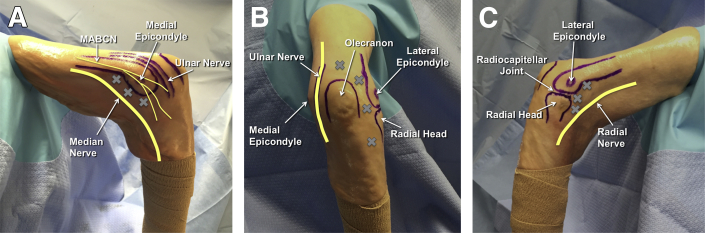
Key anatomic landmarks and surface anatomy are highlighted on a right elbow in the lateral decubitus position. (A) On the medial side, the medial epicondyle, ulnar nerve, and medial intermuscular septum should be identified. (B) When viewing the posterior aspect of the elbow, the olecranon process is easily visible. (C) Laterally, the lateral epicondyle, capitellum, radial head, and soft spot should be identified. (MABCN, medial antebrachial cutaneous nerve.)
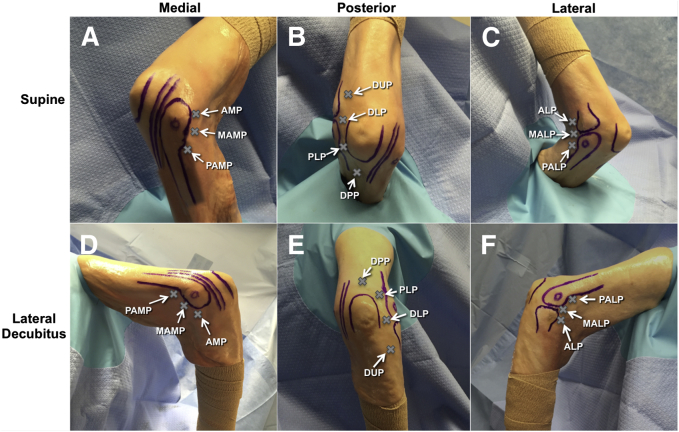
On this right elbow, the most commonly used portals for elbow arthroscopy are detailed in reference to important surrounding anatomic structures in both the supine (A-C) and lateral decubitus (D-F) positions. (A, D) From the medial side, the anteromedial portal (AMP), mid-anteromedial portal (MAMP), and proximal anteromedial portal (PAMP) can provide access to the anterior elbow. (B, E) To access the posterior elbow, the direct posterior portal (DPP), posterolateral portal (PLP), direct lateral portal (DLP), and distal ulnar portals (DUP) can be used. (C, F) Finally, the anterolateral portal (ALP), mid-anterolateral portal (MALP), and proximal anterolateral portal (PALP) can be used to access the anterior elbow joint from the lateral side.
References
-
- Guhl J.F. Arthroscopy and arthroscopic surgery of the elbow. Orthopedics. 1985;8:1290–1296. - PubMed
-
- Andrews J.R., Carson W.G. Arthroscopy of the elbow. Arthroscopy. 1985;1:97–107. - PubMed
-
- O'Driscoll S.W., Morrey B.F. Arthroscopy of the elbow. Diagnostic and therapeutic benefits and hazards. J Bone Joint Surg Am. 1992;74:84–94. - PubMed
-
- Adams J.E., King G.J., Steinmann S.P., Cohen M.S. Elbow arthroscopy: Indications, techniques, outcomes, and complications. J Am Acad Orthop Surg. 2014;22:810–818. - PubMed
-
- Dodson C.C., Nho S.J., Williams R.J., Altchek D.W. Elbow arthroscopy. J Am Acad Orthop Surg. 2008;16:574–585. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
