

Standard Pathologic Features Can Be Used to Identify a Subset of Estrogen Receptor-Positive, HER2 Negative Patients Likely to Benefit from Neoadjuvant Chemotherapy
- PMID: 28560596
- PMCID: PMC5649343
- DOI: 10.1245/s10434-017-5898-z
Standard Pathologic Features Can Be Used to Identify a Subset of Estrogen Receptor-Positive, HER2 Negative Patients Likely to Benefit from Neoadjuvant Chemotherapy
Abstract
Background: The benefit of neoadjuvant chemotherapy (NAC) in patients with estrogen receptor-positive (ER+)/human epidermal growth factor receptor 2-negative (HER2-) breast cancers and in invasive lobular carcinoma (ILC) is uncertain due to the low rates of pathologic complete response (pCR).
Objective: The aim of this study was to determine if pathologic features can identify subsets likely to benefit from NAC.
Methods: Patients with stage I-III ER+, HER2- breast cancer receiving NAC were retrospectively reviewed. Endpoints were downstaging to breast-conserving surgery (BCS) and nodal pCR after NAC. Patients were grouped by progesterone receptor (PR) status and grade/differentiation (high grade or poor [HP] vs. non-HP).
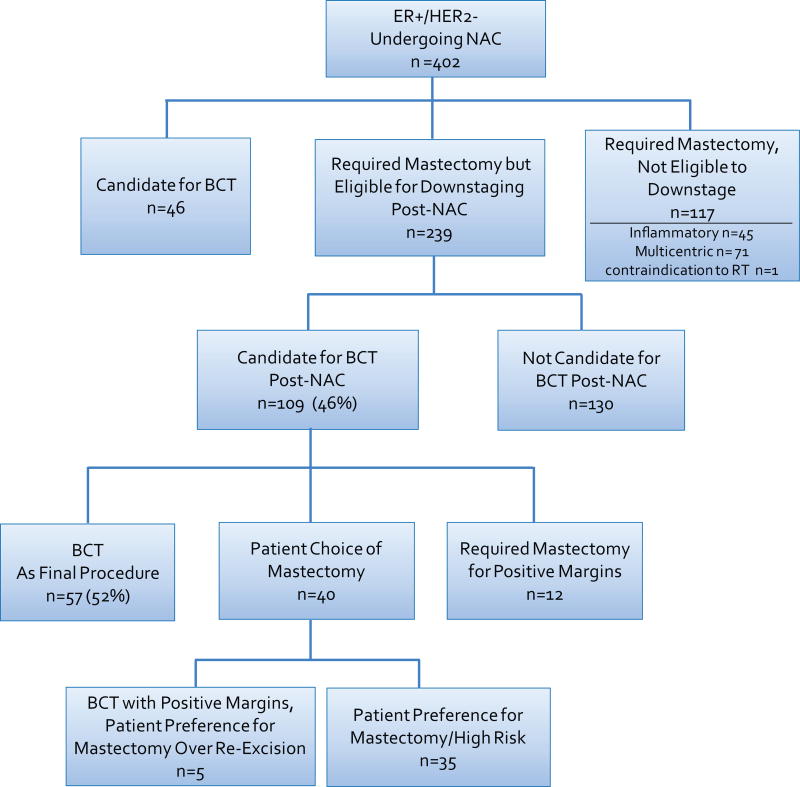
Results: From 2007 to 2016, 402 ER+/HER2- cancers in patients receiving NAC were identified. Median age was 50 years, 98% were clinical stage II-III, and 75% were cN+. Overall pCR rate was 5%; breast pCR in 7% and nodal pCR in 15% of cN+ patients (p < 0.0001). Patients with ILC initially ineligible for BCS (n = 56) were less likely to downstage than those with invasive ductal carcinoma (IDC; n = 183, 16 vs. 48%, p ≤ 0.0001), with a similar trend in the axilla (p = 0.086). The rates of BCS eligibility after NAC were highest in PR-/HP patients (62%) and lowest in PR+/non-HP patients (29%) [p = 0.005]. In the axilla, nodal pCR among cN+ patients (n = 301) ranged from 0 to 35% (p < 0.0001) within these groups, and was most frequent in PR-/HP patients.
Conclusions: ER+/HER2- patients most likely to benefit from NAC are those with PR- and HP tumors. Patients with ILC are unlikely to downstage in the breast or axilla compared with IDC. The use of these criteria can assist in defining the initial treatment approach.
Conflict of interest statement
The authors have no conflict of interest disclosures to report.
Figures
References
-
- Rastogi P, Anderson SJ, Bear HD, Geyer CE, Kahlenberg MS, Robidoux A, Margolese RG, et al. Preoperative chemotherapy: updates of National Surgical Adjuvant Breast and Bowel Project Protocols B-18 and B-27. J Clin Oncol. 2008;26(5):778–85. - PubMed
-
- van Nes JG, Putter H, Julien JP, Tubiana-Hulin M, van de Vijver M, Bogaerts J, de Vos M, et al. Preoperative chemotherapy is safe in early breast cancer, even after 10 years of follow-up; clinical and translational results from the EORTC trial 10902. Breast Cancer Res Treat. 2009;115(1):101–13. - PubMed
-
- Mieog JS, van der Hage JA, van de Velde CJ. Neoadjuvant chemotherapy for operable breast cancer. Br J Surg. 2007;94(10):1189–200. - PubMed
-
- Boughey JC, McCall LM, Ballman KV, Mittendorf EA, Ahrendt GM, Wilke LG, Taback B, et al. Tumor biology correlates with rates of breast-conserving surgery and pathologic complete response after neoadjuvant chemotherapy for breast cancer: findings from the ACOSOG Z1071 (Alliance) Prospective Multicenter Clinical Trial. Ann Surg. 2014;260(4):608–14. discussion 14-6. - PMC - PubMed
-
- Caudle AS, Yu TK, Tucker SL, Bedrosian I, Litton JK, Gonzalez-Angulo AM, Hoffman K, et al. Local-regional control according to surrogate markers of breast cancer subtypes and response to neoadjuvant chemotherapy in breast cancer patients undergoing breast conserving therapy. Breast Cancer Res. 2012;14(3):R83. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
