

The impact of a multifaceted intervention including sepsis electronic alert system and sepsis response team on the outcomes of patients with sepsis and septic shock
- PMID: 28560683
- PMCID: PMC5449351
- DOI: 10.1186/s13613-017-0280-7
The impact of a multifaceted intervention including sepsis electronic alert system and sepsis response team on the outcomes of patients with sepsis and septic shock
Abstract
Background: Compliance with the clinical practice guidelines of sepsis management has been low. The objective of our study was to describe the results of implementing a multifaceted intervention including an electronic alert (e-alert) with a sepsis response team (SRT) on the outcome of patients with sepsis and septic shock presenting to the emergency department.
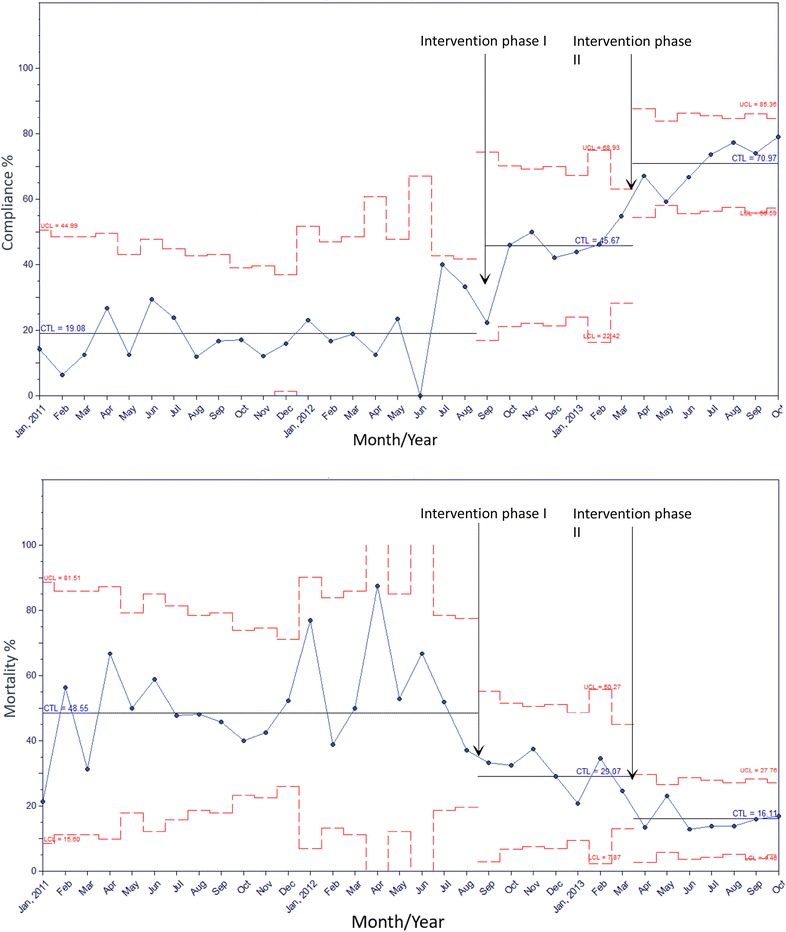
Methods: This was a pre-post two-phased implementation study that consisted of a pre-intervention phase (January 01, 2011-September 24, 2012), intervention phase I (multifaceted intervention including e-alert, from September 25, 2012-March 03, 2013) and intervention phase II when SRT was added (March 04, 2013-October 30, 2013) in a 900-bed tertiary-care academic hospital. We recorded baseline characteristics and processes of care in adult patients presenting with sepsis or septic shock. The primary outcome measures were hospital mortality. Secondary outcomes were the need for mechanical ventilation and length of stay in the intensive unit and in the hospital.
Results: After implementing the multifaceted intervention including e-alert and SRT, cases were identified with less severe clinical and laboratory abnormalities and the processes of care improved. When adjusted to propensity score, the interventions were associated with reduction in hospital mortality [for intervention phase II compared to pre-intervention: adjusted odds ratio (aOR) 0.71, 95% CI 0.58-0.85, p = 0.003], reduction in the need for mechanical ventilation (aOR 0.45, 95% CI 0.37-0.55, p < 0.0001) and reduction in ICU LOS and hospital LOS for all patients as well as ICU LOS for survivors.
Conclusions: Implementing a multifaceted intervention including sepsis e-alert with SRT was associated with earlier identification of sepsis, increase in compliance with sepsis resuscitation bundle and reduction in the need for mechanical ventilation and reduction in hospital mortality and LOS.
Keywords: Emergency department; Health service administration; Hospital mortality; Intensive care unit; Patient safety; Quality improvement; Sepsis; Sepsis resuscitation bundle; Shock.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
