

Rationale, design, and baseline characteristics of the CLARIFY registry of outpatients with stable coronary artery disease
- PMID: 28561986
- PMCID: PMC5697615
- DOI: 10.1002/clc.22730
Rationale, design, and baseline characteristics of the CLARIFY registry of outpatients with stable coronary artery disease
Abstract
Background: Despite major advances in prevention and treatment, coronary artery disease (CAD) remains the leading cause of death worldwide. Whereas many sources of data are available on the epidemiology of acute coronary syndromes, fewer datasets reflect the contemporary management and outcomes of stable CAD patients.
Hypothesis: A worldwide contemporary registry would improve our knowledge about stable CAD. The main objectives are to describe the demographics, clinical profile, contemporary management and outcomes of outpatients with stable CAD; to identify gaps between evidence and treatment; and to investigate long-term prognostic determinants.
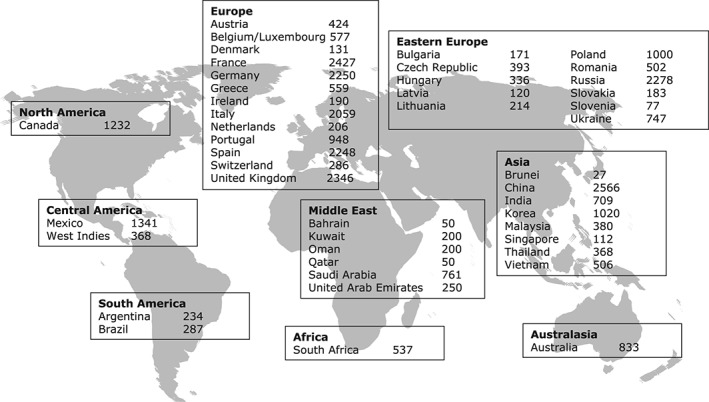
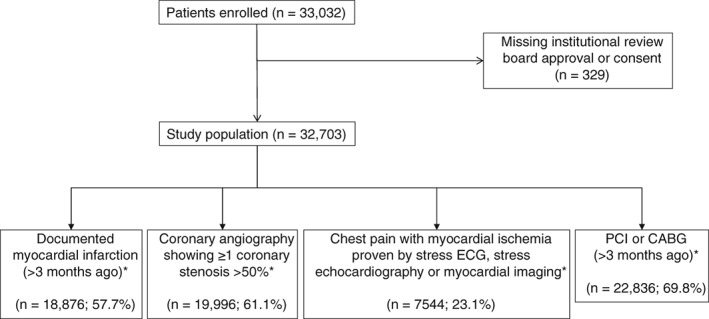
Methods: CLARIFY (ProspeCtive observational LongitudinAl RegIstry oF patients with stable coronary arterY disease) is an ongoing international observational longitudinal registry. Stable CAD patients from 45 countries in Europe, Asia, America, Middle East, Australia and Africa were enrolled between November 2009 and June 2010. The inclusion criteria were previous myocardial infarction, evidence of coronary stenosis >50%, proven symptomatic myocardial ischemia or prior revascularization procedure. The main exclusion criteria were serious non-cardiovascular disease, conditions interfering with life expectancy or severe other cardiovascular disease (including advanced heart failure). Follow-up visits were planned annually for up to 5 years, interspersed with 6-month telephone calls.
Results: Of the 32,703 patients enrolled, most (77.6%) were male, age (mean ± SD) was 64.2 ± 10.5 years, and 71.0% were receiving treatment for hypertension; mean ± SD resting heart rate was 68.2 ± 10.6 bpm. Patients were enrolled based on a history of myocardial infarction >3 months earlier (57.7%), having at least one stenosis >50% on coronary angiography (61.1%), proven symptomatic myocardial ischemia on non-invasive testing (23.1%), or history of percutaneous coronary intervention or coronary artery bypass graft (69.8%). Baseline characteristics were similar across the four subgroups identified by the four inclusion criteria.
Conclusion: CLARIFY will provide a useful resource for understanding the current epidemiology of stable CAD.
Keywords: CLARIFY Registry; Baseline Characteristics; Stable Coronary Artery Disease.
© 2017 The Authors. Clinical Cardiology published by Wiley Periodicals, Inc.
Conflict of interest statement
R.F. has served on speaker's bureau for Bayer, Merck Serono, Novartis, Amgen, Servier International, and Pfizer; discloses research grants/contracts from Boehringer Ingelheim, Novartis, Irbetch, and Servier International; has served on advisory board for Boehringer Ingelheim, Novartis, and Servier International; has received an honorarium from Servier for steering committee membership consulting and speaking plus support for travel to study meetings; has received personal fees from Boehringer‐Ingelheim, Novartis, Merck Serono, and Irbtech; and has been a stockholder in Medical Trials Analysis. I.F. discloses honoraria and research grants from Servier and Amgen. K.F. discloses honoraria and/or consultation fees and/or travel expenses from Servier, AstraZeneca, TaurX, Armgo, Broadview Ventures, and CellAegis; he is on the scientific advisory board of Celixer and is a director of Vesalius Trials Ltd. J.‐C.T. discloses research grants from Amarin, AstraZeneca, DalCor, Esperion, Ionis, Merck, Pfizer, Sanofi, and Servier, and honoraria from DalCor, Pfizer, Sanofi, and Servier. M.T. discloses honoraria and consultation fees from Servier, Bayer, Janssen‐Cilag, Celyad, and Kowa. P.G.S. discloses research grants from Merck, Sanofi, and Servier, and speaking or consulting fees from Amarin, Amgen, AstraZeneca, Bayer, Boehringer‐Ingelheim, Bristol‐Myers Squibb, CSL Behring, Daiichi Sankyo, GlaxoSmithKline, Janssen, Lilly, Merck, Novartis, Pfizer, Regeneron, Sanofi, Servier, and The Medicines Company. E.S. and N.G. have no conflicts to disclose.
Figures
References
-
- Leal J, Luengo‐Fernández R, Gray A, et al. Economic burden of cardiovascular diseases in the enlarged European Union. Eur Heart J. 2006;27:1610–1619. - PubMed
-
- Lopez AD, Mathers CD, Ezzati M, et al. Global and regional burden of disease and risk factors, 2001: systematic analysis of population health data. Lancet. 2006;367:1747–1757. - PubMed
-
- Murray CJ, Lopez AD. Alternative projections of mortality and disability by cause 1990–2020: Global Burden of Disease Study. Lancet. 1997;349:1498–1504. - PubMed
-
- Tunstall‐Pedoe H, Kuulasmaa K, Mähönen M, et al. Contribution of trends in survival and coronary‐event rates to changes in coronary heart disease mortality: 10‐year results from 37 WHO MONICA project populations. Monitoring trends and determinants in cardiovascular disease. Lancet. 1999;353:1547–1557. - PubMed
-
- Daly CA, Clemens F, López‐Sendón J, et al; Euro Heart Survey Investigators . The clinical characteristics and investigations planned in patients with stable angina presenting to cardiologists in Europe: from the Euro Heart Survey of Stable Angina. Eur Heart J. 2005;26:996–1010. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
