

Racial and Ethnic Differences in ADHD Treatment Quality Among Medicaid-Enrolled Youth
- PMID: 28562259
- PMCID: PMC5470500
- DOI: 10.1542/peds.2016-2444
Racial and Ethnic Differences in ADHD Treatment Quality Among Medicaid-Enrolled Youth
Abstract
Objectives: We estimated racial/ethnic differences in attention-deficit/hyperactivity disorder (ADHD) care quality and treatment continuity among Medicaid-enrolled children.
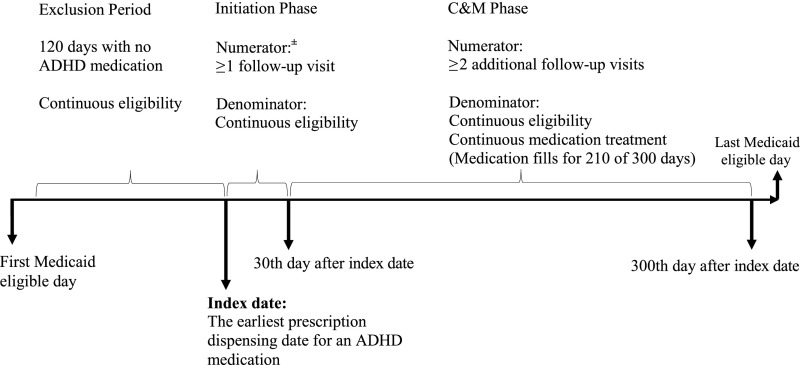
Methods: Using Medicaid data from 9 states (2008 to 2011), we identified 172 322 youth (age 6 to 12) initiating ADHD medication. Outcome measures included: (1) adequate follow-up care in the (a) initiation and (b) continuation and maintenance (C&M) treatment phases; (2) combined treatment with medication and psychotherapy (versus medication alone); (3) medication discontinuation; and (4) treatment disengagement (ie, discontinued medication and received no psychotherapy). Logistic regressions controlled for confounding measures.
Results: Among those initiating medication, three-fifths received adequate follow-up care in the initiation and C&M phases, and under two-fifths received combined treatment. Compared with whites, African American youth were less likely to receive adequate follow-up in either phase (P < .05), whereas Hispanic youth were more likely to receive adequate follow-up in the C&M phase (P < .001). African American and Hispanic youth were more likely than whites to receive combined treatment (P < .05). Over three-fifths discontinued medication, and over four-tenths disengaged from treatment. Compared with whites, African American and Hispanic children were 22.4% and 16.7% points more likely to discontinue medication, and 13.1% and 9.4% points more likely to disengage from treatment, respectively (P < .001).
Conclusions: Care quality for Medicaid-enrolled youth initiating ADHD medication is poor, and racial/ethnic differences in these measures are mixed. The most important disparities occur in the higher rates of medication discontinuation among minorities, which translate into higher rates of treatment disengagement because most youth discontinuing medication receive no psychotherapy.
Copyright © 2017 by the American Academy of Pediatrics.
Conflict of interest statement
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
Figures
Similar articles
-
Racial and Ethnic Differences in Minimally Adequate Depression Care Among Medicaid-Enrolled Youth.J Am Acad Child Adolesc Psychiatry. 2019 Jan;58(1):128-138. doi: 10.1016/j.jaac.2018.04.025. Epub 2018 Oct 17. J Am Acad Child Adolesc Psychiatry. 2019. PMID: 30577928 Free PMC article.
-
Racial-Ethnic Differences in Patterns of Discontinuous Medication Treatment Among Medicaid-Insured Youths With ADHD.Psychiatr Serv. 2018 Mar 1;69(3):322-331. doi: 10.1176/appi.ps.201600469. Epub 2017 Dec 1. Psychiatr Serv. 2018. PMID: 29191137 Free PMC article.
-
Hispanic Residential Isolation, ADHD Diagnosis and Stimulant Treatment among Medicaid-Insured Youth.Ethn Dis. 2017 Apr 20;27(2):85-94. doi: 10.18865/ed.27.2.85. eCollection 2017 Spring. Ethn Dis. 2017. PMID: 28439178 Free PMC article.
-
Diversity and representation in ADHD psychosocial treatment research: A comprehensive synthesis with data from over 10,000 participants.Clin Psychol Rev. 2024 Aug;112:102461. doi: 10.1016/j.cpr.2024.102461. Epub 2024 Jun 13. Clin Psychol Rev. 2024. PMID: 38945033 Review.
-
Challenges in ADHD care for ethnic minority children: A review of the current literature.Transcult Psychiatry. 2020 Jun;57(3):468-483. doi: 10.1177/1363461520902885. Epub 2020 Mar 31. Transcult Psychiatry. 2020. PMID: 32233772 Review.
Cited by
-
Disparities in Mental and Behavioral Health Treatment for Children and Youth in Immigrant Families.Acad Pediatr. 2020 Nov-Dec;20(8):1148-1156. doi: 10.1016/j.acap.2020.06.013. Epub 2020 Jun 26. Acad Pediatr. 2020. PMID: 32599347 Free PMC article.
-
Receipt of Addiction Treatment After Opioid Overdose Among Medicaid-Enrolled Adolescents and Young Adults.JAMA Pediatr. 2020 Mar 1;174(3):e195183. doi: 10.1001/jamapediatrics.2019.5183. Epub 2020 Mar 2. JAMA Pediatr. 2020. PMID: 31905233 Free PMC article.
-
Can We Expand the Pool of Youth Who Receive Telehealth Assessments for ADHD? Covariates of Service Utilization.J Atten Disord. 2023 Jan;27(2):159-168. doi: 10.1177/10870547221129304. Epub 2022 Oct 14. J Atten Disord. 2023. PMID: 36239415 Free PMC article.
-
Introduction to the Special Issue: Advancing Racial Justice in Clinical Child and Adolescent Psychology.J Clin Child Adolesc Psychol. 2023 May-Jun;52(3):311-327. doi: 10.1080/15374416.2023.2202255. Epub 2023 May 4. J Clin Child Adolesc Psychol. 2023. PMID: 37141558 Free PMC article. Review.
-
Association of Integrating Mental Health Into Pediatric Primary Care at Federally Qualified Health Centers With Utilization and Follow-up Care.JAMA Netw Open. 2023 Apr 3;6(4):e239990. doi: 10.1001/jamanetworkopen.2023.9990. JAMA Netw Open. 2023. PMID: 37099297 Free PMC article.
References
-
- Currie J, Stabile M. Child mental health and human capital accumulation: the case of ADHD. J Health Econ. 2006;25(6):1094–1118 - PubMed
-
- Barbaresi WJ, Katusic SK, Colligan RC, Weaver AL, Jacobsen SJ. Long-term school outcomes for children with attention-deficit/hyperactivity disorder: a population-based perspective. J Dev Behav Pediatr. 2007;28(4):265–273 - PubMed
-
- Klassen AF, Miller A, Fine S. Health-related quality of life in children and adolescents who have a diagnosis of attention-deficit/hyperactivity disorder. Pediatrics. 2004;114(5). Available at: www.pediatrics.org/cgi/content/full/114/5/e541 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
