

Widely differing screening and treatment practice for osteoporosis in patients with inflammatory bowel diseases in the Swiss IBD cohort study
- PMID: 28562531
- PMCID: PMC5459696
- DOI: 10.1097/MD.0000000000006788
Widely differing screening and treatment practice for osteoporosis in patients with inflammatory bowel diseases in the Swiss IBD cohort study
Abstract
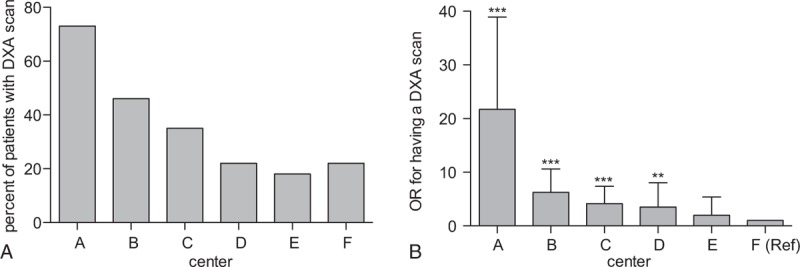
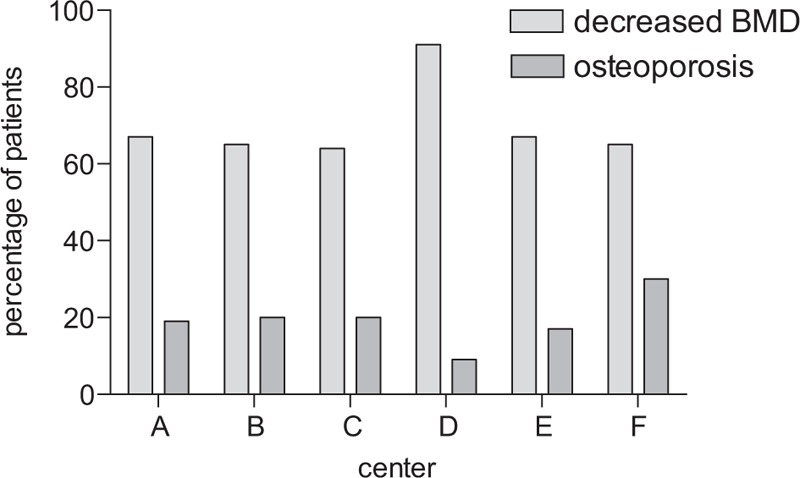
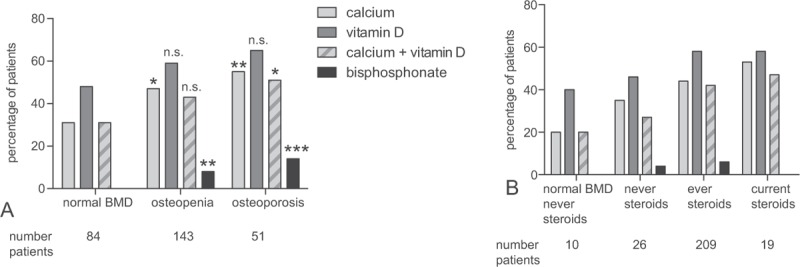
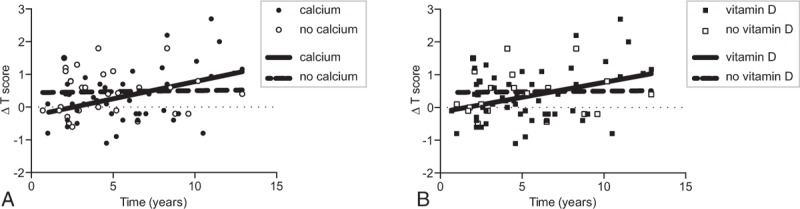
Low bone mineral density (BMD) and osteoporosis remain frequent problems in patients with inflammatory bowel diseases (IBDs). Several guidelines with nonidentical recommendations exist and there is no general agreement regarding the optimal approach for osteoporosis screening in IBD patients. Clinical practice of osteoporosis screening and treatment remains insufficiently investigated.In the year 2014, a chart review of 877 patients included in the Swiss IBD Cohort study was performed to assess details of osteoporosis diagnostics and treatment. BMD measurements, osteoporosis treatment, and IBD medication were recorded.Our chart review revealed 253 dual-energy x-ray absorptiometry (DXA) scans in 877 IBD patients; osteoporosis was prevalent in 20% of tested patients. We identified widely differing osteoporosis screening rates among centers (11%-62%). A multivariate logistic regression analysis identified predictive factors for screening including steroid usage, long disease duration, and perianal disease; even after correction for all risk factors, the study center remained a strong independent predictor (odds ratio 2.3-21 compared to the center with the lowest screening rate). Treatment rates for patients with osteoporosis were suboptimal (55% for calcium, 65% for vitamin D) at the time of chart review. Similarly, a significant fraction of patients with current steroid medication were not treated with vitamin D or calcium (treatment rates 53% for calcium, 58% for vitamin D). For only 29% of patients with osteoporosis bisphosphonate treatment was started. Treatment rates also differed among centers, generally following screening rates. In patients with longitudinal DXA scans, calcium and vitamin D usage was significantly associated with improvement of BMD over time.Our analysis identified inconsistent usage of osteoporosis screening and underuse of osteoporosis treatment in IBD patients. Increasing awareness of osteoporosis as a significant clinical problem in IBD patients might improve patient care.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Larsen S, Bendtzen K, Nielsen OH. Extraintestinal manifestations of inflammatory bowel disease: epidemiology, diagnosis, and management. Ann Med 2010;42:97–114. - PubMed
-
- Bernstein CN, Blanchard JF, Leslie W, et al. The incidence of fracture among patients with inflammatory bowel disease. A population-based cohort study. Ann Intern Med 2000;133:795–9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
