

Comparison of mid-term efficacy of spastic flatfoot in ambulant children with cerebral palsy by 2 different methods
- PMID: 28562561
- PMCID: PMC5459726
- DOI: 10.1097/MD.0000000000007044
Comparison of mid-term efficacy of spastic flatfoot in ambulant children with cerebral palsy by 2 different methods
Erratum in
-
Comparison of mid-term efficacy of spastic flatfoot in ambulant children with cerebral palsy by 2 different methods: Erratum.Medicine (Baltimore). 2018 May;97(18):e0690. doi: 10.1097/MD.0000000000010690. Medicine (Baltimore). 2018. PMID: 29718900 Free PMC article. No abstract available.
Abstract
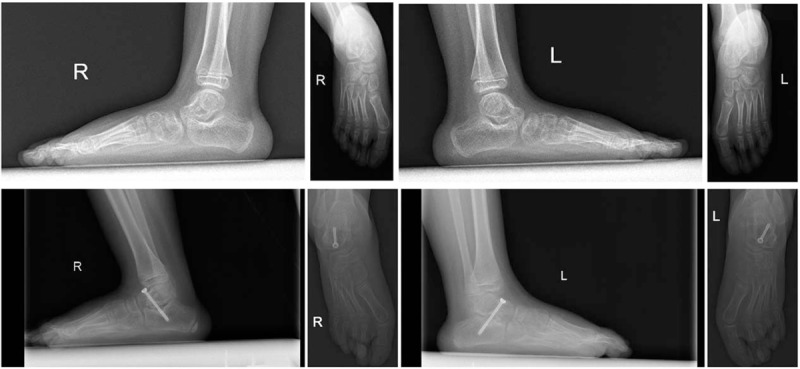
To compare the treatment efficacy of spastic flatfoot surgery by 2 different surgical methods: nonfusion subtalar arthroereisis using subtalar joint stabilizer (SJS) and Dennyson-Fulford subtalar arthrodesis (D-FSA).A total of 26 cases of ambulant children with cerebral palsy diagnosed as spastic flatfoot were surgically treated from January 2011 to December 2014. Preoperative and postoperative American Orthopedic Foot and Ankle Society-Ankle and Hindfoot (AOFAS-AH) scores, anteroposterior-talocalcaneal angles (ATAs), and lateral talar-first metatarsal angles (Meary angles) of the affected foot were recorded.Among 12 children in the SJS group, the AOFAS-AH scores were median preoperative score of 61 (58-64) versus median postoperative score of 83 (75-92), with significant difference (P < .05). Of the 20 feet treated, only 1 foot developed occasional pain. Postoperative ATA was decreased from preoperative 35° (20°-50°) to 19° (12°-25°); lateral X-ray films showed that the Meary angle was decreased from preoperative 20° (15°-40°) to postoperative 0° (0°-3°). The differences in both findings were statistically significant (P < .05). Fourteen children (22 treated feet) formed the D-FSA group; all demonstrated fusion of the talocalcaneal joint; AOFAS-AH scores were median preoperative score of 61 (58-64) versus median postoperative score of 83 (75-92), with significant difference (P < .05). Only 1 foot had occasional pain. Postoperative ATA was decreased from preoperative 35° (20°-45°) to 16° (12°-25°); lateral X-ray films showed that the Meary angle was decreased from preoperative 19° (10°-40°) to postoperative 2° (0°-5°); the differences in both findings were statistically significant (P < .05).Both nonfusion subtalar arthroereisis using SJS and D-FSA were effective for the surgical treatment of spastic flatfoot, with similar clinical outcomes.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures


Similar articles
-
Lateral column lengthening versus subtalar arthroereisis for paediatric flatfeet: a systematic review.Int Orthop. 2019 May;43(5):1179-1192. doi: 10.1007/s00264-019-04303-3. Epub 2019 Jan 30. Int Orthop. 2019. PMID: 30701302
-
Mid-term Results of Subtalar Arthroereisis with Talar-Fit Implant in Pediatric Flexible Flatfoot and Identifying the Effects of Adjunctive Procedures and Risk Factors for Sinus Tarsi Pain.Orthop Surg. 2021 Feb;13(1):175-184. doi: 10.1111/os.12864. Epub 2020 Dec 17. Orthop Surg. 2021. PMID: 33332772 Free PMC article.
-
Therapeutic Outcomes of Kalix II in Treating Juvenile Flexible Flatfoot.Orthop Surg. 2017 Feb;9(1):20-27. doi: 10.1111/os.12309. Orthop Surg. 2017. PMID: 28371501 Free PMC article.
-
Preliminary Results of Calcaneal Lengthening Osteotomy Combined With Extra-articular Subtalar Arthrodesis for Severe Pes Planovalgus Deformity in Children With Cerebral Palsy: A New Surgical Technique.J Pediatr Orthop. 2024 Aug 1;44(7):e647-e656. doi: 10.1097/BPO.0000000000002698. Epub 2024 Apr 16. J Pediatr Orthop. 2024. PMID: 38623033
-
Subtalar arthroereisis combined with medial soft tissue reconstruction in treating pediatric flexible flatfoot with accessory navicular.J Orthop Surg Res. 2023 Jan 19;18(1):55. doi: 10.1186/s13018-023-03542-w. J Orthop Surg Res. 2023. PMID: 36658597 Free PMC article. Review.
Cited by
-
Radiological outcome after treatment of juvenile flatfeet with subtalar arthroereisis: a matched pair analysis of 38 cases comparing neurogenic and non-neurogenic patients.J Child Orthop. 2019 Aug 1;13(4):346-352. doi: 10.1302/1863-2548.13.190046. J Child Orthop. 2019. PMID: 31489039 Free PMC article.
-
Lateral column lengthening versus subtalar arthroereisis for pes planovalgus in patients with cerebral palsy: a systematic review and meta-analysis.Front Pediatr. 2024 Sep 18;12:1443447. doi: 10.3389/fped.2024.1443447. eCollection 2024. Front Pediatr. 2024. PMID: 39359741 Free PMC article.
-
Surgical management of pes planus in children with cerebral palsy: A systematic review.J Child Orthop. 2022 Oct;16(5):333-346. doi: 10.1177/18632521221112496. Epub 2022 Sep 2. J Child Orthop. 2022. PMID: 36238147 Free PMC article. Review.
-
Lateral column lengthening versus subtalar arthroereisis for paediatric flatfeet: a systematic review.Int Orthop. 2019 May;43(5):1179-1192. doi: 10.1007/s00264-019-04303-3. Epub 2019 Jan 30. Int Orthop. 2019. PMID: 30701302
-
Subtalar arthroereisis for treatment of children with flexible planovalgus foot deformity and analysis of CT data in long-term period.J Orthop. 2020 Oct 8;22:478-484. doi: 10.1016/j.jor.2020.10.005. eCollection 2020 Nov-Dec. J Orthop. 2020. PMID: 33093758 Free PMC article.
References
-
- Miller F. Cerebral Palsy-Section I, Part 11: Knee, Leg and Foot. 2004;New York, NY: Springer, 667–802.
-
- Duffy C, Cosgrove A. The foot in cerebral palsy. Curr Orthop 2002;16:104–13.
-
- Patterson RL, Jr, Parrish FF, Hathaway EN. Stabilizing operations on the foot; a study of the indications, techniques used, and end results. J Bone Joint Surg Am 1950;32A:1–26. - PubMed
-
- Aiona MD, Sussman MD. Treatment of spastic diplegia in patients with cerebral palsy: part II. J Pediatr Orthop B 2004;13:S13–38. - PubMed
-
- Morrell DS, Pearson JM, Sauser DD. Progressive bone and joint abnormalities of the spine and lower extremities in cerebral palsy. Radiographics 2002;22:257–68. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
