

The Metabolic Phenotype in Obesity: Fat Mass, Body Fat Distribution, and Adipose Tissue Function
- PMID: 28564650
- PMCID: PMC5644968
- DOI: 10.1159/000471488
The Metabolic Phenotype in Obesity: Fat Mass, Body Fat Distribution, and Adipose Tissue Function
Abstract
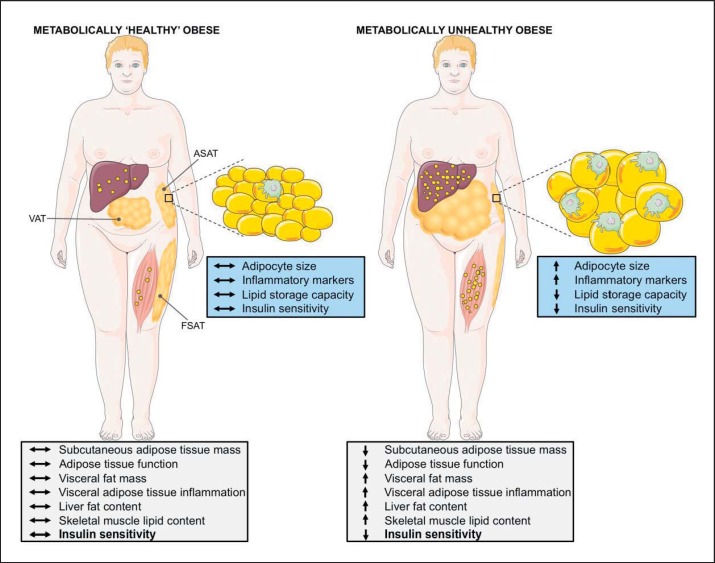
The current obesity epidemic poses a major public health issue since obesity predisposes towards several chronic diseases. BMI and total adiposity are positively correlated with cardiometabolic disease risk at the population level. However, body fat distribution and an impaired adipose tissue function, rather than total fat mass, better predict insulin resistance and related complications at the individual level. Adipose tissue dysfunction is determined by an impaired adipose tissue expandability, adipocyte hypertrophy, altered lipid metabolism, and local inflammation. Recent human studies suggest that adipose tissue oxygenation may be a key factor herein. A subgroup of obese individuals - the 'metabolically healthy obese' (MHO) - have a better adipose tissue function, less ectopic fat storage, and are more insulin sensitive than obese metabolically unhealthy persons, emphasizing the central role of adipose tissue function in metabolic health. However, controversy has surrounded the idea that metabolically healthy obesity may be considered really healthy since MHO individuals are at increased (cardio)metabolic disease risk and may have a lower quality of life than normal weight subjects due to other comorbidities. Detailed metabolic phenotyping of obese persons will be invaluable in understanding the pathophysiology of metabolic disturbances, and is needed to identify high-risk individuals or subgroups, thereby paving the way for optimization of prevention and treatment strategies to combat cardiometabolic diseases.
Keywords: Adipose tissue function; Body fat; Metabolic health; Obesity; Oxygen.
© 2017 The Author(s) Published by S. Karger GmbH, Freiburg.
Figures
References
-
- Kopelman PG. Obesity as a medical problem. Nature. 2000;404:635–643. - PubMed
-
- Kahn SE. The relative contributions of insulin resistance and beta-cell dysfunction to the pathophysiology of type 2 diabetes. Diabetologia. 2003;46:3–19. - PubMed
-
- Bergman RN, Ader M, Huecking K, Van Citters G. Accurate assessment of beta-cell function: the hyperbolic correction. Diabetes. 2002;51(suppl 1):S212–220. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
