

Association Between Skin and Aortic Vascular Inflammation in Patients With Psoriasis: A Case-Cohort Study Using Positron Emission Tomography/Computed Tomography
- PMID: 28564678
- PMCID: PMC5815046
- DOI: 10.1001/jamacardio.2017.1213
Association Between Skin and Aortic Vascular Inflammation in Patients With Psoriasis: A Case-Cohort Study Using Positron Emission Tomography/Computed Tomography
Abstract
Importance: Inflammation is critical in the development of atherosclerosis. Psoriasis is a chronic inflammatory skin disease that is associated with increased vascular inflammation by 18fluorodeoxyglucose positron emission tomography/computed tomography in vivo and future cardiovascular events. It provides a human model to understand the effect of treating inflammation in a target organ (eg, the skin) on vascular diseases.
Objective: To investigate the association between change in skin disease severity and change in vascular inflammation at 1 year and to characterize the impact of 1 year of anti-tumor necrosis factor therapy on vascular inflammation.
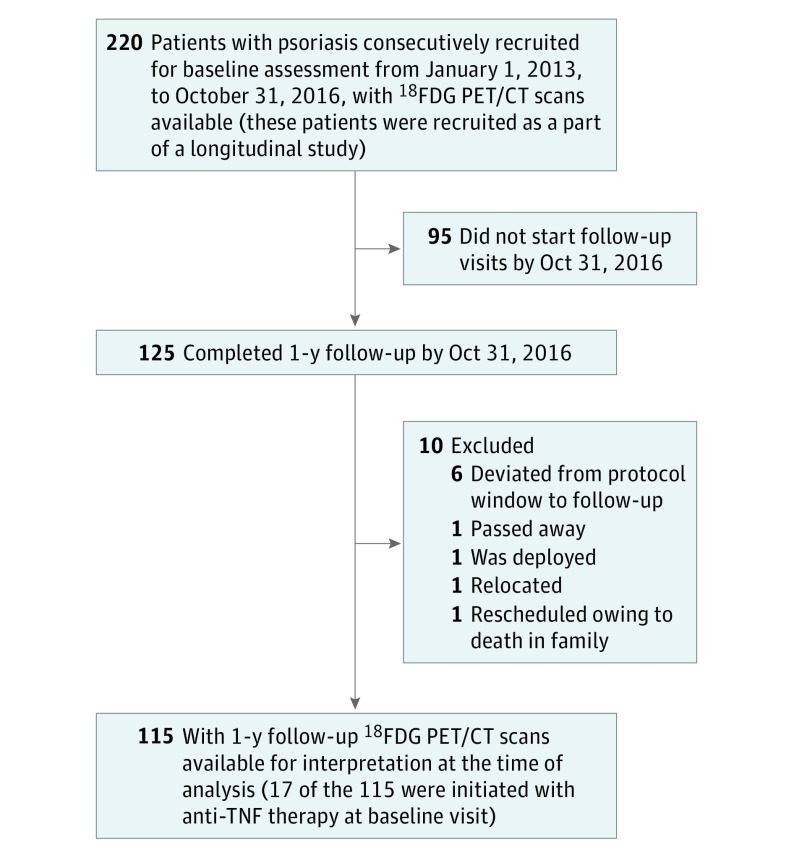
Design, setting, and participants: In this prospective cohort study, 220 participants from outpatient practices were recruited at the US National Institutes of Health. A total of 115 consecutively recruited patients with psoriasis were followed up at 1 year. The study was conducted from January 1, 2013, through October 31, 2016, with data analyzed in November 2016.
Exposure: Skin inflammation measured as Psoriasis Area and Severity Index (PASI) score.
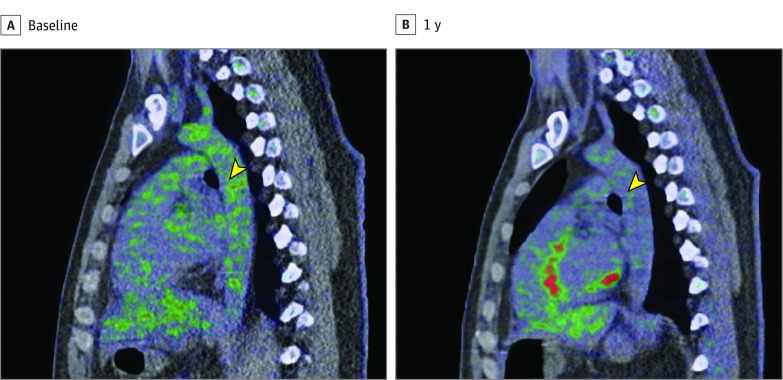
Main outcomes and measures: Vascular inflammation assessed as target-to-background ratio by 18fluorodeoxyglucose positron emission tomography/computed tomography.
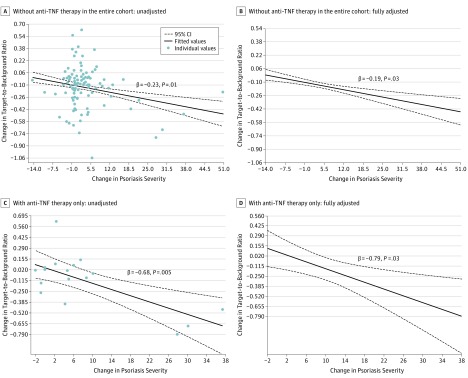
Results: Among the 115 patients, the mean (SD) age at 1-year follow-up was 50.8 (12.8) years and 68 were men (59%). The cohort had a low cardiovascular risk by Framingham risk score and mild-to-moderate psoriasis, with a median PASI score of 5.2 (interquartile range, 3.0-8.9). At follow-up, the total cohort had a median improvement in PASI score of 33%, with use of topical therapy (60%), biological therapy (66%, mostly anti-tumor necrosis factor) and phototherapy (15%) (P < .001). Moreover, improvement in PASI score was associated with improvement in target-to-background ratio of 6%, mainly driven by those with higher responses in PASI score (P < .001). This association persisted beyond traditional risk factors (β = 0.19; 95% CI, 0.012-0.375; P = .03) and was the strongest in those initiated with anti-tumor necrosis factor therapy (β = 0.79; 95% CI, 0.269-1.311; P = .03).
Conclusions and relevance: Improvement in psoriasis skin disease severity was associated with improvement in aortic vascular inflammation by 18fluorodeoxyglucose positron emission tomography/computed tomography, with greater improvement in aortic vascular inflammation observed in those who had higher than 75% reduction in skin disease severity. These findings suggest that controlling remote target organ inflammation (eg, in the skin) may improve vascular diseases; however, randomized clinical trials are needed to confirm these findings.
Conflict of interest statement
Figures
Comment in
-
Skin and Vascular Disease-Inside-Out/Outside-In.JAMA Cardiol. 2017 Sep 1;2(9):944-945. doi: 10.1001/jamacardio.2017.1420. JAMA Cardiol. 2017. PMID: 28564684 No abstract available.
References
-
- Gelfand JM, Neimann AL, Shin DB, Wang X, Margolis DJ, Troxel AB. Risk of myocardial infarction in patients with psoriasis. JAMA. 2006;296(14):1735-1741. - PubMed
-
- Ahlehoff O, Gislason GH, Lindhardsen J, et al. Prognosis following first-time myocardial infarction in patients with psoriasis: a Danish nationwide cohort study. J Intern Med. 2011;270(3):237-244. - PubMed
-
- Figueroa AL, Abdelbaky A, Truong QA, et al. Measurement of arterial activity on routine FDG PET/CT images improves prediction of risk of future CV events. JACC Cardiovasc Imaging. 2013;6(12):1250-1259. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
