

High Level of Integration in Integrated Disease Management Leads to Higher Usage in the e-Vita Study: Self-Management of Chronic Obstructive Pulmonary Disease With Web-Based Platforms in a Parallel Cohort Design
- PMID: 28566268
- PMCID: PMC5471344
- DOI: 10.2196/jmir.7037
High Level of Integration in Integrated Disease Management Leads to Higher Usage in the e-Vita Study: Self-Management of Chronic Obstructive Pulmonary Disease With Web-Based Platforms in a Parallel Cohort Design
Abstract
Background: Worldwide, nearly 3 million people die of chronic obstructive pulmonary disease (COPD) every year. Integrated disease management (IDM) improves disease-specific quality of life and exercise capacity for people with COPD, but can also reduce hospital admissions and hospital days. Self-management of COPD through eHealth interventions has shown to be an effective method to improve the quality and efficiency of IDM in several settings, but it remains unknown which factors influence usage of eHealth and change in behavior of patients.
Objective: Our study, e-Vita COPD, compares different levels of integration of Web-based self-management platforms in IDM in three primary care settings. The main aim of this study is to analyze the factors that successfully promote the use of a self-management platform for COPD patients.
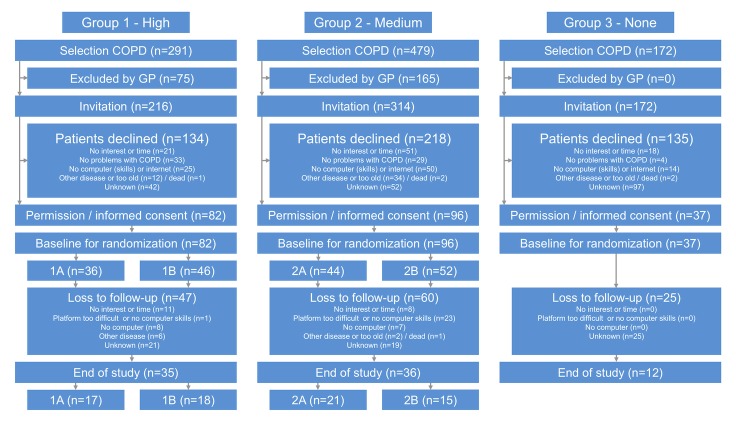
Methods: The e-Vita COPD study compares three different approaches to incorporating eHealth via Web-based self-management platforms into IDM of COPD using a parallel cohort design. Three groups integrated the platforms to different levels. In groups 1 (high integration) and 2 (medium integration), randomization was performed to two levels of personal assistance for patients (high and low assistance); in group 3 there was no integration into disease management (none integration). Every visit to the e-Vita and Zorgdraad COPD Web platforms was tracked objectively by collecting log data (sessions and services). At the first log-in, patients completed a baseline questionnaire. Baseline characteristics were automatically extracted from the log files including age, gender, education level, scores on the Clinical COPD Questionnaire (CCQ), dyspnea scale (MRC), and quality of life questionnaire (EQ5D). To predict the use of the platforms, multiple linear regression analyses for the different independent variables were performed: integration in IDM (high, medium, none), personal assistance for the participants (high vs low), educational level, and self-efficacy level (General Self-Efficacy Scale [GSES]). All analyses were adjusted for age and gender.
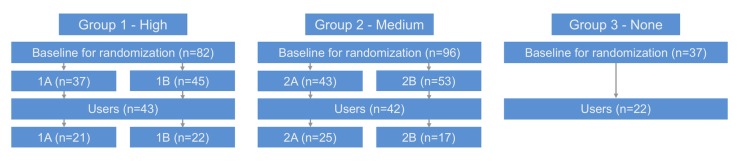
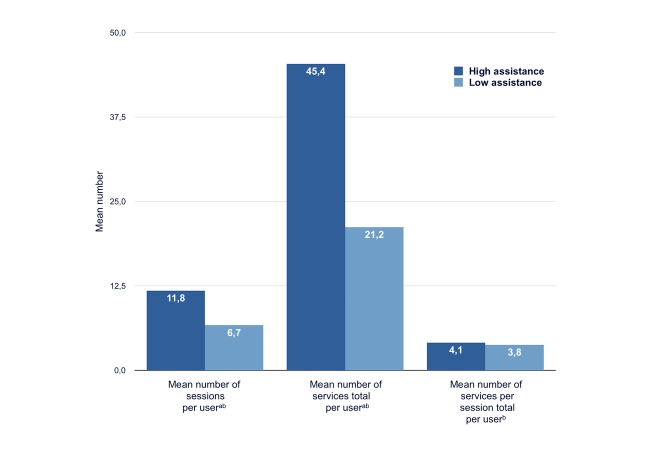
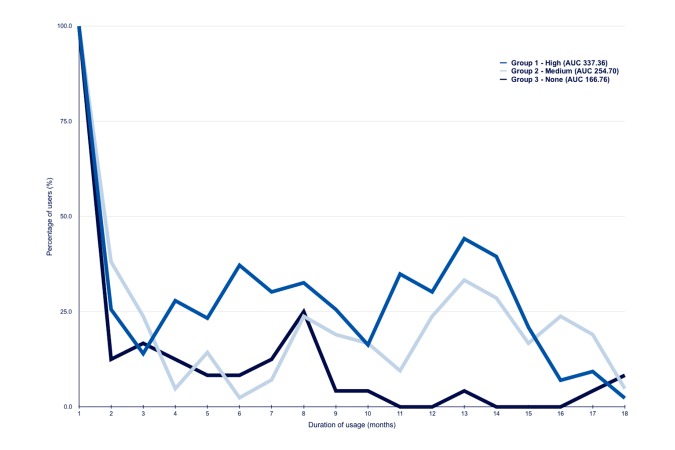
Results: Of the 702 invited COPD patients, 215 (30.6%) registered to a platform. Of the 82 patients in group 1 (high integration IDM), 36 were in group 1A (personal assistance) and 46 in group 1B (low assistance). Of the 96 patients in group 2 (medium integration IDM), 44 were in group 2A (telephone assistance) and 52 in group 2B (low assistance). A total of 37 patients participated in group 3 (no integration IDM). In all, 107 users (49.8%) visited the platform at least once in the 15-month period. The mean number of sessions differed between the three groups (group 1: mean 10.5, SD 1.3; group 2: mean 8.8, SD 1.4; group 3: mean 3.7, SD 1.8; P=.01). The mean number of sessions differed between the high-assistance and low-assistance groups in groups 1 and 2 (high: mean 11.8, SD 1.3; low: mean 6.7, SD 1.4; F1,80=6.55, P=.01). High-assistance participants used more services (mean 45.4, SD 6.2) than low-assistance participants (mean 21.2, SD 6.8; F1,80=6.82, P=.01). No association was found between educational level and usage and between GSES and usage.
Conclusions: Use of a self-management platform is higher when participants receive adequate personal assistance about how to use the platform. Blended care, where digital health and usual care are integrated, will likely lead to increased use of the online program. Future research should provide additional insights into the preferences of different patient groups.
Trial registration: Nederlands Trial Register NTR4098; http://www.trialregister.nl/trialreg/admin/rctview.asp?TC=4098 (Archived by WebCite at http://www.webcitation.org/6qO1hqiJ1).
Keywords: COPD; Web-based platform; blended care; chronically ill; eHealth; integrated disease management; primary care; self-efficacy; self-management.
©Esther PWA Talboom-Kamp, Noortje A Verdijk, Marise J Kasteleyn, Lara M Harmans, Irvin JSH Talboom, Mattijs E Numans, Niels H Chavannes. Originally published in the Journal of Medical Internet Research (http://www.jmir.org), 31.05.2017.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures


Similar articles
-
The Effect of Integration of Self-Management Web Platforms on Health Status in Chronic Obstructive Pulmonary Disease Management in Primary Care (e-Vita Study): Interrupted Time Series Design.J Med Internet Res. 2017 Aug 16;19(8):e291. doi: 10.2196/jmir.8262. J Med Internet Res. 2017. PMID: 28814380 Free PMC article.
-
e-Vita: design of an innovative approach to COPD disease management in primary care through eHealth application.BMC Pulm Med. 2016 Aug 16;16(1):121. doi: 10.1186/s12890-016-0282-5. BMC Pulm Med. 2016. PMID: 27530775 Free PMC article. Clinical Trial.
-
Effects of use of an eHealth platform e-Vita for COPD patients on disease specific quality of life domains.Respir Res. 2019 Jul 10;20(1):146. doi: 10.1186/s12931-019-1110-2. Respir Res. 2019. PMID: 31291945 Free PMC article.
-
Effectiveness of Digital Health Interventions for Chronic Obstructive Pulmonary Disease: Systematic Review and Meta-Analysis.J Med Internet Res. 2025 May 26;27:e76323. doi: 10.2196/76323. J Med Internet Res. 2025. PMID: 40418567 Free PMC article.
-
The State of the Art of eHealth Self-Management Interventions for People With Chronic Obstructive Pulmonary Disease: Scoping Review.J Med Internet Res. 2025 Mar 10;27:e57649. doi: 10.2196/57649. J Med Internet Res. 2025. PMID: 40063949 Free PMC article.
Cited by
-
Adherence to Telemonitoring by Electronic Patient-Reported Outcome Measures in Patients with Chronic Diseases: A Systematic Review.Int J Environ Res Public Health. 2021 Sep 27;18(19):10161. doi: 10.3390/ijerph181910161. Int J Environ Res Public Health. 2021. PMID: 34639463 Free PMC article.
-
Usefulness and Relevance of an eHealth Tool in Supporting the Self-Management of Chronic Obstructive Pulmonary Disease: Explorative Qualitative Study of a Cocreative Process.JMIR Hum Factors. 2018 Oct 26;5(4):e10801. doi: 10.2196/10801. JMIR Hum Factors. 2018. PMID: 30368440 Free PMC article.
-
The Impact of Participant Characteristics on Use and Satisfaction of a Web-Based Computer-Tailored Chronic Obstructive Pulmonary Disease Self-Management Intervention: A Process Evaluation.JMIR Form Res. 2017 Aug 21;1(1):e1. doi: 10.2196//formative.6585. JMIR Form Res. 2017. PMID: 30684399 Free PMC article.
-
The Impact of Patient Characteristics on Their Attitudes Toward an Online Patient Portal for Communicating Laboratory Test Results: Real-World Study.JMIR Form Res. 2021 Dec 17;5(12):e25498. doi: 10.2196/25498. JMIR Form Res. 2021. PMID: 34927593 Free PMC article.
-
A TASMAN Expedition: Development of a Questionnaire to Assess Specific Self-Management Abilities.Int J Chron Obstruct Pulmon Dis. 2020 Jun 19;15:1415-1423. doi: 10.2147/COPD.S224943. eCollection 2020. Int J Chron Obstruct Pulmon Dis. 2020. PMID: 32606650 Free PMC article.
References
-
- Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, Abraham J, Adair T, Aggarwal R, Ahn SY, Alvarado M, Anderson HR, Anderson LM, Andrews KG, Atkinson C, Baddour LM, Barker-Collo S, Bartels DH, Bell ML, Benjamin EJ, Bennett D, Bhalla K, Bikbov B, Bin AA, Birbeck G, Blyth F, Bolliger I, Boufous S, Bucello C, Burch M, Burney P, Carapetis J, Chen H, Chou D, Chugh SS, Coffeng LE, Colan SD, Colquhoun S, Colson KE, Condon J, Connor MD, Cooper LT, Corriere M, Cortinovis M, de Vaccaro KC, Couser W, Cowie BC, Criqui MH, Cross M, Dabhadkar KC, Dahodwala N, Degenhardt L, Delossantos A, Denenberg J, Des Jarlais DC, Dharmaratne SD, Dorsey ER, Driscoll T, Duber H, Ebel B, Erwin PJ, Espindola P, Ezzati M, Feigin V, Flaxman AD, Forouzanfar MH, Fowkes FG, Franklin R, Fransen M, Freeman MK, Gabriel SE, Gakidou E, Gaspari F, Gillum RF, Gonzalez-Medina D, Halasa YA, Haring D, Harrison JE, Havmoeller R, Hay RJ, Hoen B, Hotez PJ, Hoy D, Jacobsen KH, James SL, Jasrasaria R, Jayaraman S, Johns N, Karthikeyan G, Kassebaum N, Keren A, Khoo J, Knowlton LM, Kobusingye O, Koranteng A, Krishnamurthi R, Lipnick M, Lipshultz SE, Ohno SL, Mabweijano J, MacIntyre MF, Mallinger L, March L, Marks GB, Marks R, Matsumori A, Matzopoulos R, Mayosi BM, McAnulty JH, McDermott MM, McGrath J, Mensah GA, Merriman TR, Michaud C, Miller M, Miller TR, Mock C, Mocumbi AO, Mokdad AA, Moran A, Mulholland K, Nair MN, Naldi L, Narayan KM, Nasseri K, Norman P, O'Donnell M, Omer SB, Ortblad K, Osborne R, Ozgediz D, Pahari B, Pandian JD, Rivero AP, Padilla RP, Perez-Ruiz F, Perico N, Phillips D, Pierce K, Pope CA, Porrini E, Pourmalek F, Raju M, Ranganathan D, Rehm JT, Rein DB, Remuzzi G, Rivara FP, Roberts T, De León FR, Rosenfeld LC, Rushton L, Sacco RL, Salomon JA, Sampson U, Sanman E, Schwebel DC, Segui-Gomez M, Shepard DS, Singh D, Singleton J, Sliwa K, Smith E, Steer A, Taylor JA, Thomas B, Tleyjeh IM, Towbin JA, Truelsen T, Undurraga EA, Venketasubramanian N, Vijayakumar L, Vos T, Wagner GR, Wang M, Wang W, Watt K, Weinstock MA, Weintraub R, Wilkinson JD, Woolf AD, Wulf S, Yeh P, Yip P, Zabetian A, Zheng Z, Lopez AD, Murray CJ, AlMazroa MA, Memish ZA. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012 Dec 15;380(9859):2095–2128. doi: 10.1016/S0140-6736(12)61728-0. - DOI - PMC - PubMed
-
- World Health Organization. 2015. Mar, [2015-10-17]. Chronic obstructive pulmonary disease (COPD): fact sheet http://www.who.int/mediacentre/factsheets/fs315/en/ 6lKKYMcI5
-
- Global Initiative for Chronic Obstructive Pulmonary Disease. 2016. [2016-10-17]. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease http://goldcopd.org/ 6lKKjGL5q
-
- Bellamy D, Bouchard J, Henrichsen S, Johansson G, Langhammer A, Reid J, van Weel C, Buist S. International Primary Care Respiratory Group (IPCRG) Guidelines: management of chronic obstructive pulmonary disease (COPD) Prim Care Respir J. 2006 Feb;15(1):48–57. doi: 10.1016/j.pcrj.2005.11.003. doi: 10.1016/j.pcrj.2005.11.003. - DOI - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
