

Infected nonunion of tibia
- PMID: 28566776
- PMCID: PMC5439310
- DOI: 10.4103/ortho.IJOrtho_199_16
Infected nonunion of tibia
Abstract
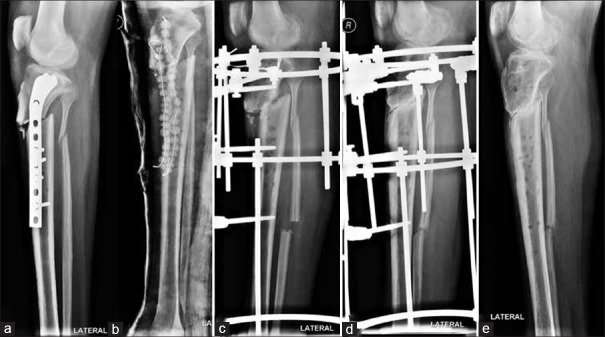
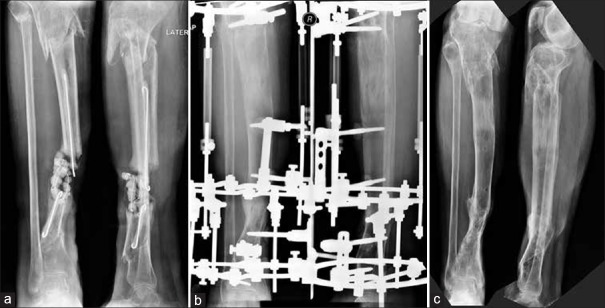
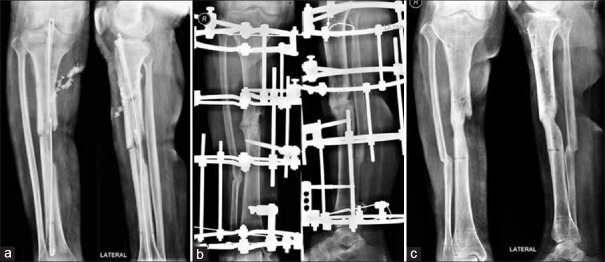
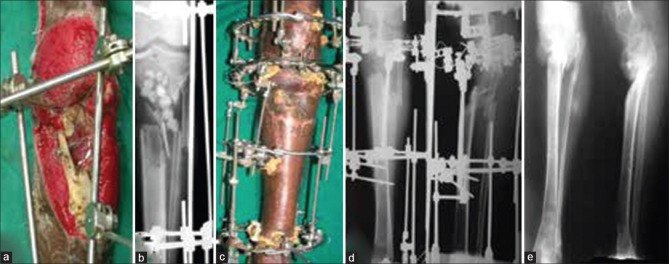
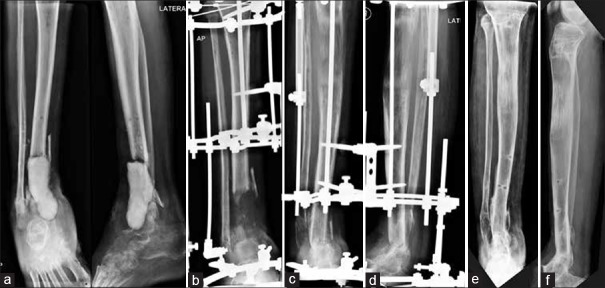
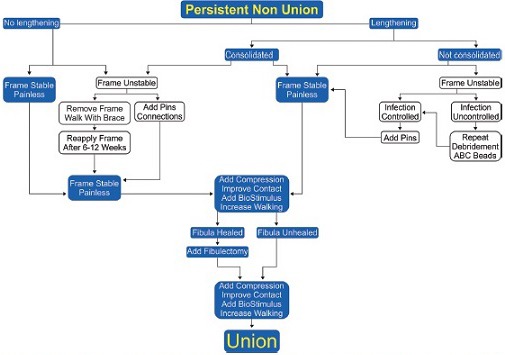
Infected nonunions of tibia pose many challenges to the treating surgeon and the patient. Challenges include recalcitrant infection, complex deformities, sclerotic bone ends, large bone gaps, shortening, and joint stiffness. They are easy to diagnose and difficult to treat. The ASAMI classification helps decide treatment. The nonunion severity score proposed by Calori measures many parameters to give a prognosis. The infection severity score uses simple clinical signs to grade severity of infection. This determines number of surgeries and allows choice of hardware, either external or internal for definitive treatment. Co-morbid factors such as smoking, diabetes, nonsteroidal anti-inflammatory drug use, and hypovitaminosis D influence the choice and duration of treatment. Thorough debridement is the mainstay of treatment. Removal of all necrotic bone and soft tissue is needed. Care is exercised in shaping bone ends. Internal fixation can help achieve union if infection was mild. Severe infections need external fixation use in a second stage. Compression at nonunion site achieves union. It can be combined with a corticotomy lengthening at a distant site for equalization. Soft tissue deficit has to be covered by flaps, either local or microvascular. Bone gaps are best filled with the reliable technique of bone transport. Regenerate bone may be formed proximally, distally, or at both sites. Acute compression can fill bone gaps and may need a fibular resection. Gradual reduction of bone gap happens with bone transport, without need for fibulectomy. When bone ends dock, union may be achieved by vertical or horizontal compression. Biological stimulus from iliac crest bone grafts, bone marrow aspirate injections, and platelet concentrates hasten union. Bone graft substitutes add volume to graft and help fill defects. Addition of rh-BMP-7 may help in healing albeit at a much higher cost. Regeneration may need stimulation and augmentation. Induced membrane technique is an alternative to bone transport to fill gaps. It needs large amounts of bone graft from iliac crest or femoral canal. This is an expensive method physiologically and economically. Infection can resorb the graft and cause failure of treatment. It can be done in select cases after thorough eradication of infection. Patience and perseverance are needed for successful resolution of infection and achieving union.
Keywords: Bone cements; Infection; antibiotic cement; bone diseases; bone regeneration; bone transport; gap nonunion; induced membrane technique; infection severity score; infections; nonunion; regenerate bone; tibia.
Conflict of interest statement
There are no conflicts of interest.
Figures


References
-
- Keating JF, Simpson AH, Robinson CM. The management of fractures with bone loss. J Bone Joint Surg Br. 2005 Feb;87(2):142–50. - PubMed
-
- Bose D, Kugan R, Stubbs D, McNally M. Management of infected nonunion of the long bones by a multidisciplinary team. Bone Joint J. 2015;97-B:814–7. - PubMed
-
- Dendrinos GK, Kontos S, Lyritsis E. Use of the Ilizarov technique for treatment of nonunion of the tibia associated with infection. J Bone Joint Surg Am. 1995;77:835–46. - PubMed
-
- Mora R, Pedrotti L, Bertani B, Quattrini F. Treatment of infected nonunions. In: Mora R, editor. Nonunion of the Long Bones: Diagnosis and Treatment with Compression-Distraction Techniques. New York: Springer; 2006. pp. 199–223.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous