

Assessment of Fetal Development Using Cardiac Valve Intervals
- PMID: 28567021
- PMCID: PMC5434138
- DOI: 10.3389/fphys.2017.00313
Assessment of Fetal Development Using Cardiac Valve Intervals
Abstract
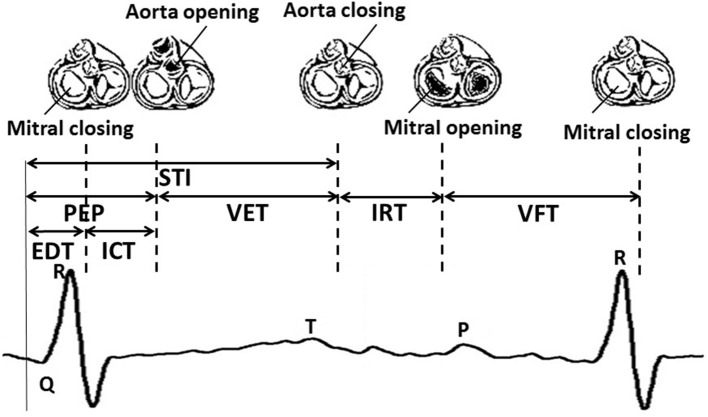
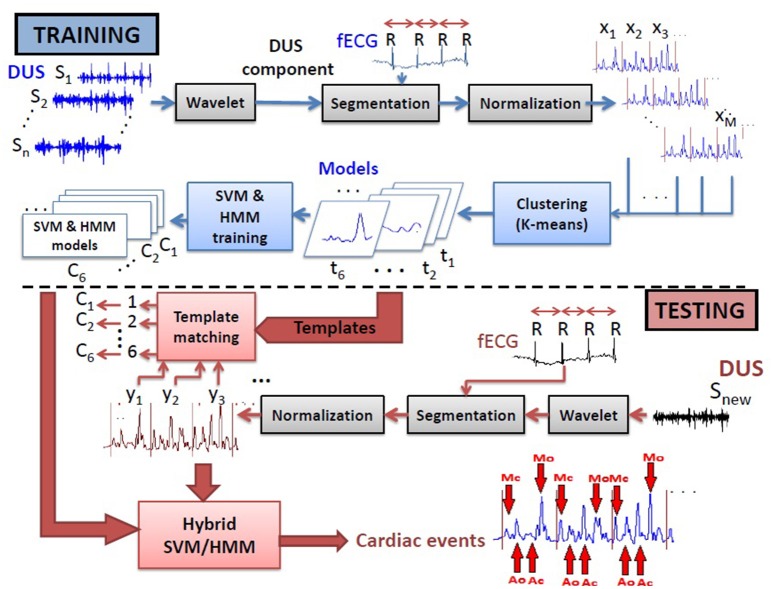
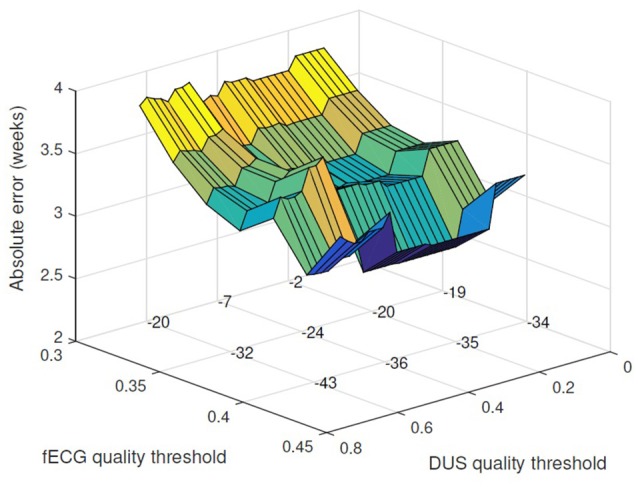
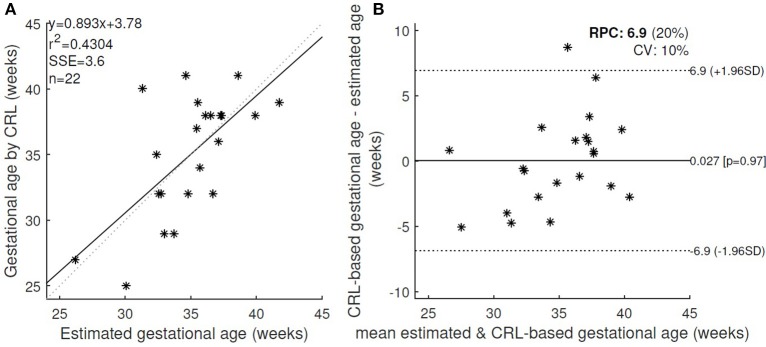
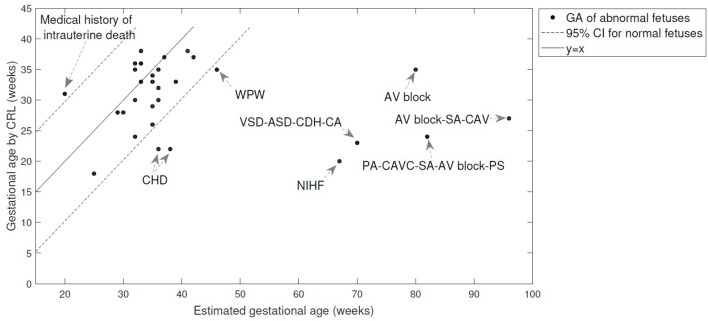
An automated method to assess the fetal physiological development is introduced which uses the component intervals between fetal cardiac valve timings and the Q-wave of fetal electrocardiogram (fECG). These intervals were estimated automatically from one-dimensional Doppler Ultrasound and noninvasive fECG. We hypothesize that the fetal growth can be estimated by the cardiac valve intervals. This hypothesis was evaluated by modeling the fetal development using the cardiac intervals and validating against the gold standard gestational age identified by Crown-Rump Length (CRL). Among the intervals, electromechanical delay time, isovolumic contraction time, ventricular filling time and their interactions were selected in a stepwise regression process that used gestational age as the target in a cohort of 57 fetuses. Compared with the gold standard age, the newly proposed regression model resulted in a mean absolute error of 3.8 weeks for all recordings and 2.7 weeks after excluding the low quality recordings. Since Fetal Heart Rate Variability (FHRV) has been proposed in the literature for assessing the fetal development, we compared the performance of gestational age estimation by our new valve-interval based method, vs. FHRV, while assuming the CRL as the gold standard. The valve interval-based method outperformed both the model based on FHRV. Results of evaluation for 30 abnormal cases showed that the new method is less affected by arrhythmias such as tachycardia and bradycardia compared to FHRV, however certain types of heart anomalies cause large errors (more than 10 weeks) with respect to the CRL-based gold standard age. Therefore, discrepancies between the regression based estimation and CRL age estimation could indicate the abnormalities. The cardiac valve intervals have been known to reflect the autonomic function. Therefore the new method potentially provides a novel approach for assessing the development of fetal autonomic nervous system, which may be growth curve independent.
Keywords: 1D Doppler ultrasound; autonomic nervous system (ANS); cardiotocography (CTG); fetal development; fetal electrocardiography (fECG); fetal monitoring; gestational age; systolic and diastolic time intervals.
Figures
References
-
- Abuhamad A. Z., Chaoui R. (2012). A Practical Guide to Fetal Echocardiography: Normal and Abnormal Hearts. Philadelphia, PA: Lippincott Williams & Wilkins.
-
- Al-Amin A., Hingston T., Mayall P., Araujo Júnior E., Fabrício Da Silva C., Friedman D. (2015). The utility of ultrasound in late pregnancy compared with clinical evaluation in detecting small and large for gestational age fetuses in low-risk pregnancies. J. Maternal-Fetal Neonatal Med. 28, 1495–1499. 10.3109/14767058.2014.961007 - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources