

Bilateral persistent primitive hypoglossal arteries associated with unilateral symptomatic carotid thromboembolism
- PMID: 28567180
- PMCID: PMC5439450
- DOI: 10.3941/jrcr.v11i4.3010
Bilateral persistent primitive hypoglossal arteries associated with unilateral symptomatic carotid thromboembolism
Abstract
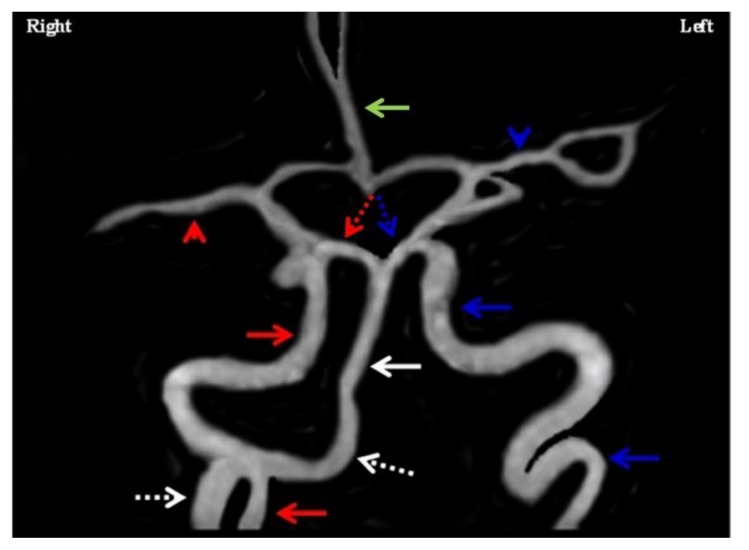
We report the fifth case of bilateral persistent primitive hypoglossal arteries in the literature. This is also the first such case to be demonstrated on computerized tomography angiogram (CTA) and the first case to be associated with a symptomatic carotid thrombus. The sub-occlusive thrombus was distal to the take-off of the dominant persistent hypoglossal artery (PHA) from the internal carotid artery, thus sparing involvement of posterior circulation. Timely identification of the internal carotid artery thromboembolism in the setting of a PHA is important to allow for thrombectomy. Any intervention was not done in this case as the patient was out of the window and at an additional risk of inducing intracranial thromboembolism. Symptomatic carotid stenosis at the PHA take-off is typically treated with endovascular angioplasty and stenting due to the typically high level of the bifurcation in the neck.
Keywords: Bilateral persistent hypoglossal artery; carotid thromboembolism; computed tomography angiogram; endovascular stenting; fetal variant.
Figures





References
-
- Uchino A, Saito N, Okada Y, Kozawa E, Nishi N, Mizukoshi W, Inoue K, Nakajima R, Takahashi M. Persistent hypoglossal artery and its variants diagnosed by CT and MR angiography. Neuroradiology. 2013 Jan 1;55(1):17–23. - PubMed
-
- Karasawa J, Kikuchi HA, Furuse SE, Sakaki TO, Yoshida YA, Ohnishi HI. Bilateral persistent carotid-basilar anastomoses. American Journal of Roentgenology. 1976 Dec 1;127(6):1053–6. - PubMed
-
- Murayama Y, Fujimoto N, Matsumoto K. Bilateral persistent primitive hypoglossal arteries associated with a large ruptured aneurysm on one side. Surgical neurology. 1985 Nov 30;24(5):498–502. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources