

Abnormal brain metabolism on FDG-PET/CT is a common early finding in autoimmune encephalitis
- PMID: 28567435
- PMCID: PMC5442608
- DOI: 10.1212/NXI.0000000000000352
Abnormal brain metabolism on FDG-PET/CT is a common early finding in autoimmune encephalitis
Abstract
Objective: To compare the rate of abnormal brain metabolism by FDG-PET/CT to other paraclinical findings and to describe brain metabolism patterns in autoimmune encephalitis (AE).
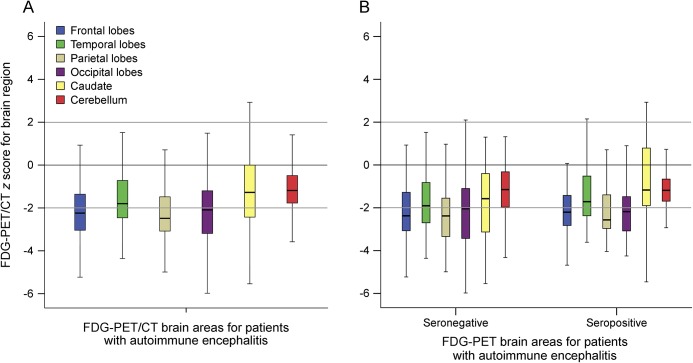
Methods: A retrospective review of clinical data and initial dedicated brain FDG-PET/CT studies for neurology inpatients with AE, per consensus criteria, treated at a single tertiary center over 123 months. Z-score maps of FDG-PET/CT were made using 3-dimensional stereotactic surface projections with comparison to age group-matched controls. Brain region mean Z-scores with magnitudes ≥2.00 were interpreted as significant. Comparisons were made to rates of abnormal initial brain MRI, abnormal initial EEG, and presence of intrathecal inflammation.
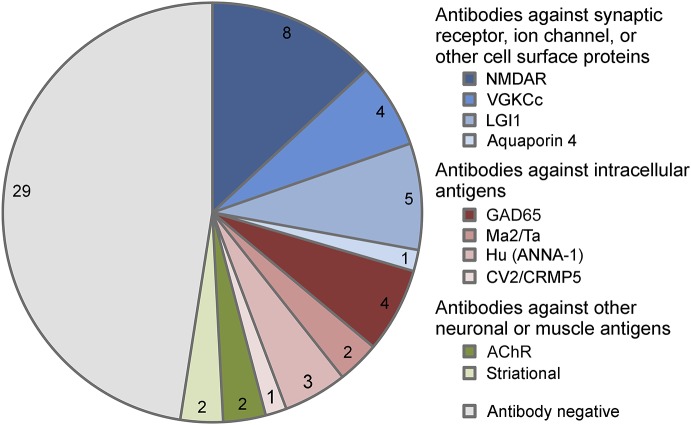
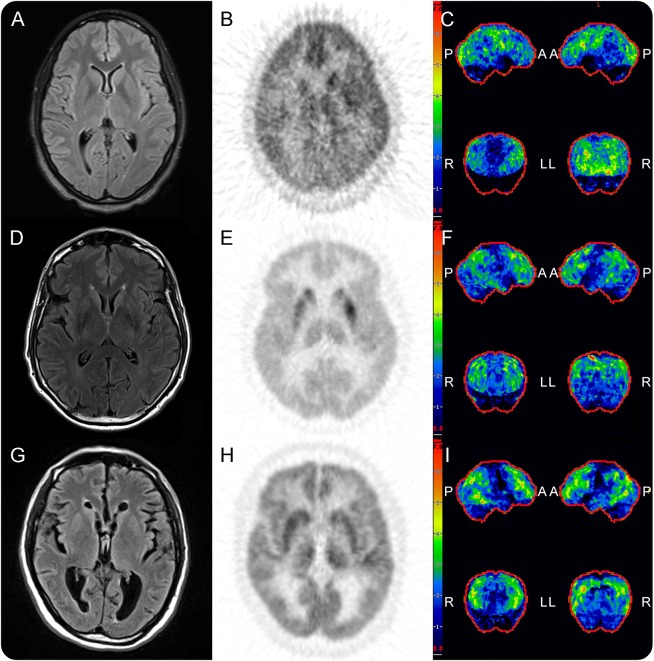
Results: Sixty-one patients with AE (32 seropositive) underwent brain FDG-PET/CT at median 4 weeks of symptoms (interquartile range [IQR] 9 weeks) and median 4 days from MRI (IQR 8.5 days). FDG-PET/CT was abnormal in 52 (85%) patients, with 42 (69%) demonstrating only hypometabolism. Isolated hypermetabolism was demonstrated in 2 (3%) patients. Both hypermetabolic and hypometabolic brain regions were noted in 8 (13%) patients. Nine (15%) patients had normal FDG-PET/CT studies. CSF inflammation was evident in 34/55 (62%) patients, whereas initial EEG (17/56, 30%) and MRI (23/57, 40%) were abnormal in fewer. Detection of 2 or more of these paraclinical findings was in weak agreement with abnormal brain FDG-PET/CT (κ = 0.16, p = 0.02).
Conclusions: FDG-PET/CT was more often abnormal than initial EEG, MRI, and CSF studies in neurology inpatients with AE, with brain region hypometabolism the most frequently observed.
Figures
References
-
- Fisher RE, Patel NR, Lai EC, Schulz PE. Two different 18F-FDG brain PET metabolic patterns in autoimmune limbic encephalitis. Clin Nucl Med 2012;37:e213–e218. - PubMed
-
- Baumgartner A, Rauer S, Mader I, Meyer PT. Cerebral FDG-PET and MRI findings in autoimmune limbic encephalitis: correlation with autoantibody types. J Neurol 2013;260:2744–2753. - PubMed
-
- Masangkay N, Basu S, Moghbel M, Kwee T, Alavi A. Brain 18F-FDG-PET characteristics in patients with paraneoplastic neurological syndrome and its correlation with clinical and MRI findings. Nucl Med Commun 2014;35:1038–1046. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources