

Mirizzi syndrome: a new insight provided by a novel classification
- PMID: 28567449
- PMCID: PMC5449366
- DOI: 10.14701/ahbps.2017.21.2.67
Mirizzi syndrome: a new insight provided by a novel classification
Abstract
Backgrounds/aims: Mirizzi syndrome (MS) is an uncommon complication of cholelithiasis. The aim of this study is to evaluate our 15-year experience in this challenging entity and to propose a new classification for this disease.
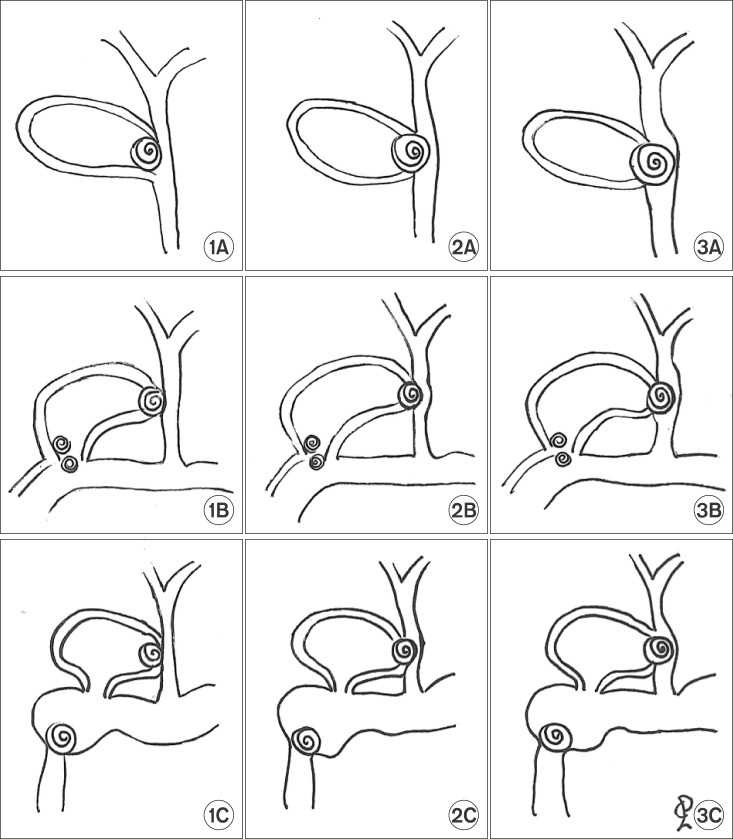
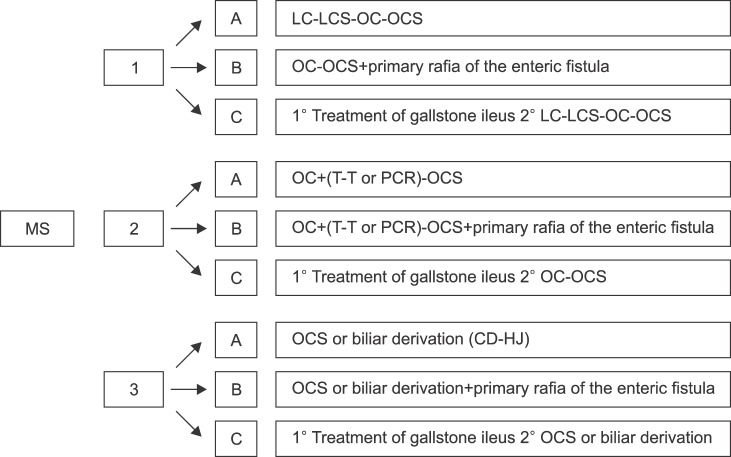
Methods: A retrospective study including patients diagnosed with Mirizzi syndrome and undergoing surgical procedures for Mirizzi syndrome between January 2000 and October 2015 was conducted. Data collected included clinical, surgical procedure, postoperative morbidity. Patients were evaluated according to the Csendes classification and the proposed system, in which patients were divided into three types and three subtypes.
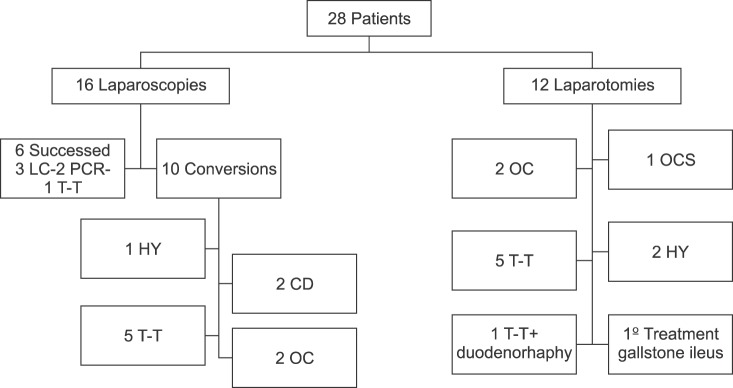
Results: 28 patients were included for analysis. They accounted as the 0.5% of a total of 4853 cholecystectomies performed in the study period. There were 21 women and 7 men. Initial laparotomic approach was performed in 12 patients and in 16 patients laparoscopic procedures were attempted. The procedure was completed in only 6 patients, 5 presenting type I and 1 type II Mirizzi syndrome. Mean postoperative stay was 15±9 days. Postoperative morbidity rate was 28%. Postoperative mortality was none.
Conclusions: Laparoscopic surgery for Mirizzi syndrome has been shown succesful only in early stages. A novel classification is proposed, based on the types of common bile duct injuries and in the presence cholecystoenteric fistula.
Keywords: Cholecystectomy; Cholecystoenteric fistula; Cholelithiasis; Mirizzi syndrome.
Figures
References
-
- Kehr H. Die in neiner klinik geubte technik de gallenstein operationen, mit einen hinweis auf die indikationen und die dauerersolge. Munchen: JF Lehman; 1905.
-
- Ruge E. Deitrage zur chirurgischen anatomie der grossen galenwege (Ductus hepaticus, choledochus, und pancreaticus) Arch Clin Chir. 1908;78:47.
-
- Abou-Saif A, Al-Kawas FH. Complications of gallstone disease: Mirizzi syndrome, cholecystocholedochal fistula, and gallstone ileus. Am J Gastroenterol. 2002;97:249–254. - PubMed
-
- Mirizzi PL. Physiologic sphincter of the hepatic bile duct. Arch Surg. 1940;41:1325–1333.
-
- Mirizzi PL. Sindrome del conducto hepatico. J Int Chir. 1948;8:731–777.
LinkOut - more resources
Full Text Sources
Other Literature Sources