

Gene therapy for monogenic liver diseases: clinical successes, current challenges and future prospects
- PMID: 28567541
- PMCID: PMC5500673
- DOI: 10.1007/s10545-017-0053-3
Gene therapy for monogenic liver diseases: clinical successes, current challenges and future prospects
Abstract
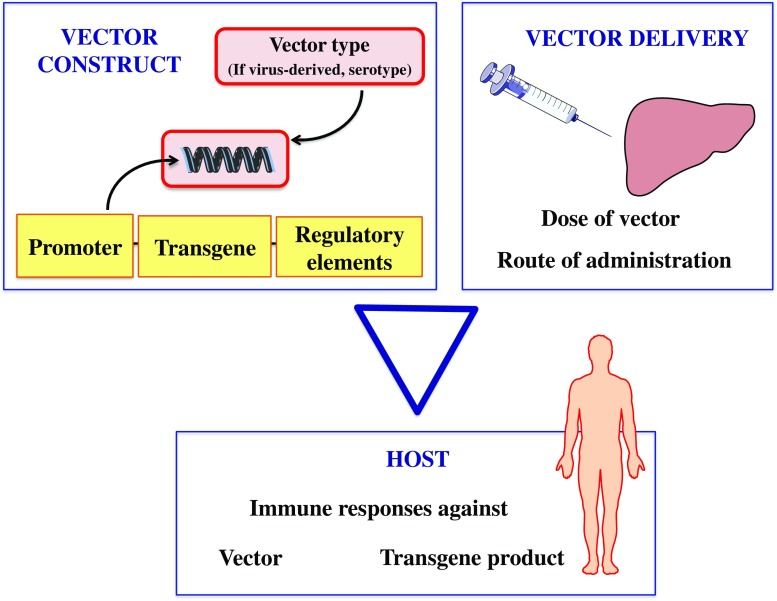
Over the last decade, pioneering liver-directed gene therapy trials for haemophilia B have achieved sustained clinical improvement after a single systemic injection of adeno-associated virus (AAV) derived vectors encoding the human factor IX cDNA. These trials demonstrate the potential of AAV technology to provide long-lasting clinical benefit in the treatment of monogenic liver disorders. Indeed, with more than ten ongoing or planned clinical trials for haemophilia A and B and dozens of trials planned for other inherited genetic/metabolic liver diseases, clinical translation is expanding rapidly. Gene therapy is likely to become an option for routine care of a subset of severe inherited genetic/metabolic liver diseases in the relatively near term. In this review, we aim to summarise the milestones in the development of gene therapy, present the different vector tools and their clinical applications for liver-directed gene therapy. AAV-derived vectors are emerging as the leading candidates for clinical translation of gene delivery to the liver. Therefore, we focus on clinical applications of AAV vectors in providing the most recent update on clinical outcomes of completed and ongoing gene therapy trials and comment on the current challenges that the field is facing for large-scale clinical translation. There is clearly an urgent need for more efficient therapies in many severe monogenic liver disorders, which will require careful risk-benefit analysis for each indication, especially in paediatrics.
Conflict of interest statement
Conflict of interest
J. Baruteau, S. N. Waddington, I. E. Alexander, and P. Gissen declare that they have no conflict of interest.
Funding
J.B. is funded by Action Medical Research for Children Charity (grant GN2137) and Great Ormond Street Hospital (GOSH) Children’s Charity Clinical Research Starter Grant. J.B., S.N.W. and P.G. are in receipt of the UK Medical Research Council (MRC) grant MR/N019075/1. S.N.W. is funded by the MRC grants MR/N026101/1 and MR/P026494/1.
Figures



References
-
- Alba R, Bosch A, Chillon M. Gutless adenovirus: last-generation adenovirus for gene therapy. Gene Ther. 2005;12(Suppl 1):S18–S27. - PubMed
-
- Andrews JL, Kadan MJ, Gorziglia MI, Kaleko M, Connelly S. Generation and characterization of E1/E2a/E3/E4-deficient adenoviral vectors encoding human factor VIII. Mol Ther. 2001;3:329–336. - PubMed
-
- Angelis A, Tordrup D, Kanavos P. Socio-economic burden of rare diseases: a systematic review of cost of illness evidence. Health Policy. 2015;119:964–979. - PubMed
-
- Annoni A, Goudy K, Akbarpour M, Naldini L, Roncarolo MG. Immune responses in liver-directed lentiviral gene therapy. Transl Res. 2013;161:230–240. - PubMed
-
- Apolonia L, Waddington SN, Fernandes C, et al. Stable gene transfer to muscle using non-integrating lentiviral vectors. Mol Ther. 2007;15:1947–1954. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
