

Dysfunctional voiding: the importance of non-invasive urodynamics in diagnosis and treatment
- PMID: 28567611
- PMCID: PMC5799351
- DOI: 10.1007/s00467-017-3679-3
Dysfunctional voiding: the importance of non-invasive urodynamics in diagnosis and treatment
Abstract
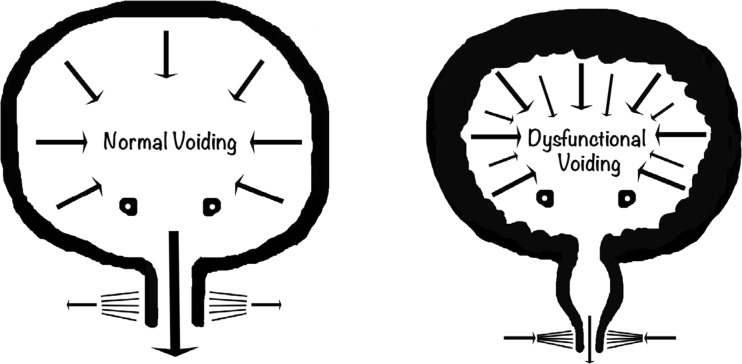
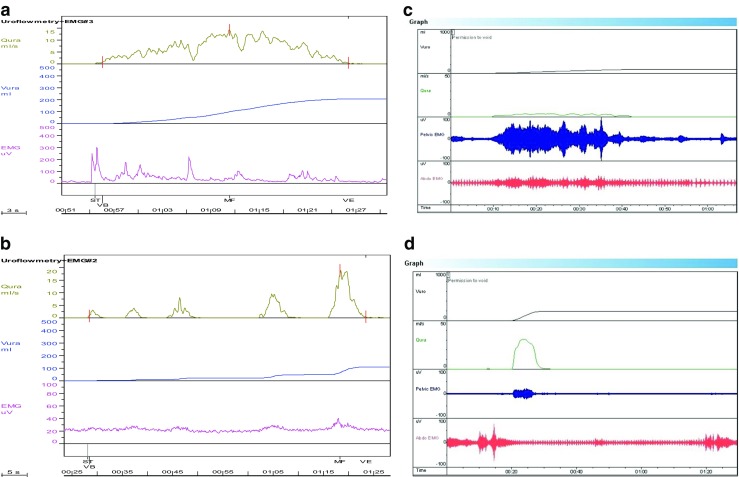
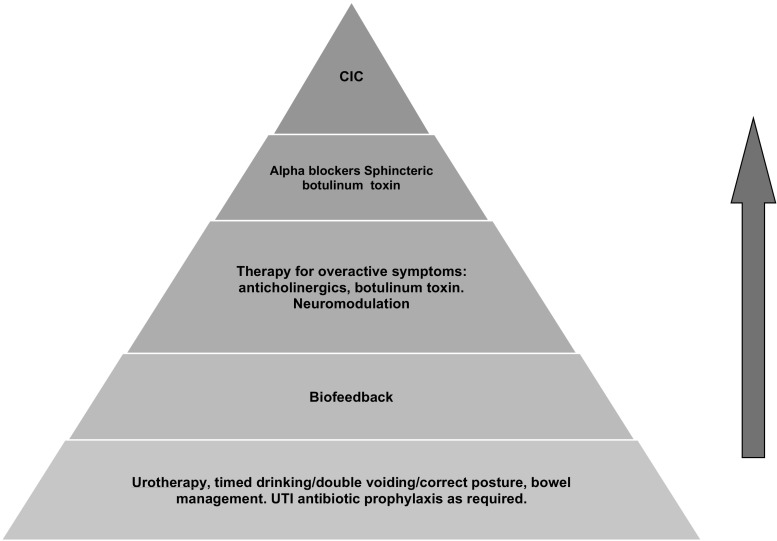
In Dysfunctional voiding, failure of the external sphincter-pelvic floor complex to relax during micturition results in bladder outflow obstruction with a spectrum of presentation from more benign lower urinary tract dysfunction including recurrent urinary tract infections, to significant upper tract pathology and end-stage renal failure. There is no underlying neurological or anatomical cause and the condition is postulated to be a largely learnt behavior. Diagnosis relies on non-invasive urodynamics and in particular uroflowmetry, plus or minus EMG, which is also used in biofeedback, the mainstay of treatment. The etiology, presentation, diagnosis, and treatment with particular emphasis on non-invasive urodynamics are covered.
Keywords: Dysfunctional voiding; Lower urinary tract dysfunction; Pelvic floor; Urinary tract infection; Uroflowmetry EMG.
Conflict of interest statement
Conflict of interest
The authors declare no conflicts of interest.
Disclosures
Dr Joanna Clothier has no disclosures to make.
Dr Anne Wright is a member of the Data Safety Monitoring Board for clinical studies of Mirabegron in children and adolescents sponsored by Astellas Pharma Europe B.V.
Figures
References
-
- Austin PF, Bauer SB, Bower W, Chase J, Franco I, Hoebeke P, Rittig S, Vande Walle J, von Gontard A, Wright A, Yang SS, Neveus T. The standardization of terminology of lower urinary tract function in children and adolescents: update report from the standardization Committee of the International Children’s Continence Society. Neurourol Urodyn. 2016;35(4):471–481. doi: 10.1002/nau.22751. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
