

The prevalence of ACPA is lower in rheumatoid arthritis patients with an older age of onset but the composition of the ACPA response appears identical
- PMID: 28569212
- PMCID: PMC5452396
- DOI: 10.1186/s13075-017-1324-y
The prevalence of ACPA is lower in rheumatoid arthritis patients with an older age of onset but the composition of the ACPA response appears identical
Abstract
Background: Rheumatoid arthritis (RA) consists of two syndromes, one autoantibody-positive and one autoantibody-negative. Existing data on the relation between age of onset and prevalence of autoantibodies were conflicting. Therefore this multicohort study assessed the age of onset in relation to the presence of autoantibodies. The association with characteristics of the anti-citrullinated protein antibodies (ACPA) response was also explored.
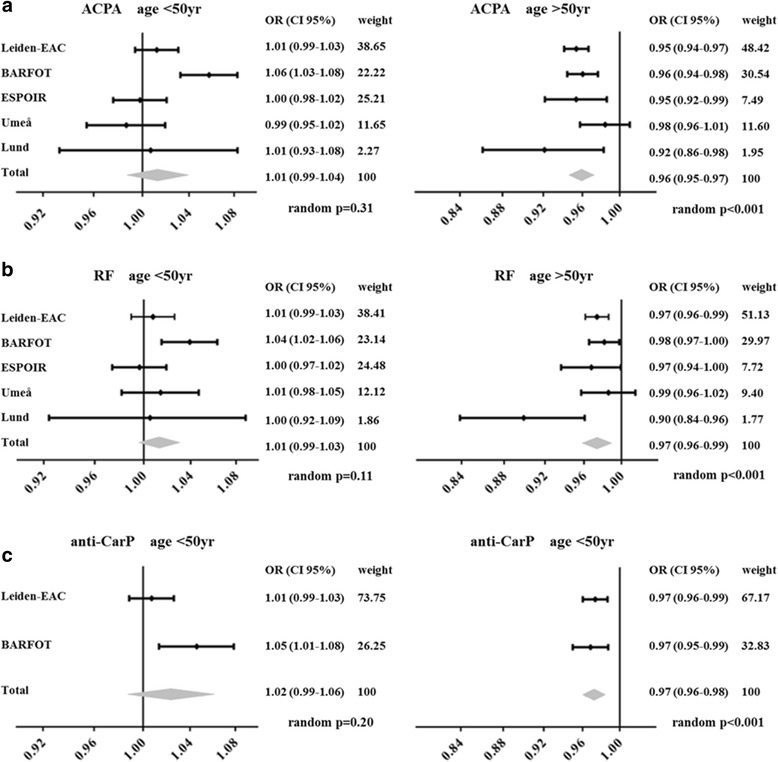
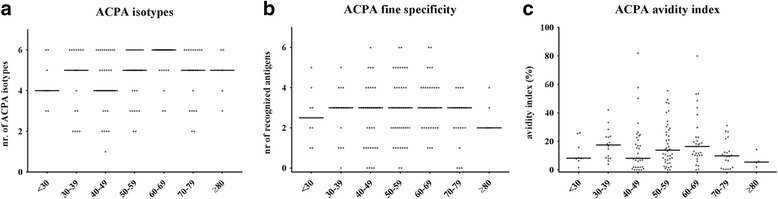
Methods: The 1987 criteria-positive RA patients included in the Leiden EAC, BARFOT, ESPOIR, Umeå and Lund cohorts (n = 3321) were studied at presentation for age of onset and the presence of ACPA, rheumatoid factor (RF) and anti-carbamylated protein (anti-CarP) antibodies. Logistic regression analyses were performed; effect sizes were summarized in inverse-weighted meta-analyses. Within ACPA-positive RA, ACPA level was studied in all cohorts; ACPA isotypes, ACPA fine specificity and ACPA avidity index and clinical characteristics were studied in the Leiden EAC.
Results: From the age of 50 onward, the proportion of ACPA-negative RA patients increased with age in the five cohorts. Similar observations were made for RF and anti-CarP. The composition of the ACPA response did not change with increasing age of onset with respect to titer, isotype distribution, fine specificity and avidity index. With increasing age of onset, RA patients smoked less often, had higher acute phase reactants and more often had a sub(acute) symptom onset.
Conclusions: Data of five cohorts revealed that with older age of onset ACPA-negative RA is more frequent than ACPA-positive RA, while characteristics of ACPA-positive RA as judged by the composition of the ACPA response appeared not age dependent. Further biologic studies are needed to characterize the pathogenesis of ACPA-negative polyarthritis at older age and to promote personalized treatment decisions in ACPA-negative patients in daily practice.
Keywords: ACPA characteristics; Age; Autoantibodies; Rheumatoid arthritis.
Figures



References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
