

A clinically validated prediction method for facial soft-tissue changes following double-jaw surgery
- PMID: 28570001
- PMCID: PMC5553697
- DOI: 10.1002/mp.12391
A clinically validated prediction method for facial soft-tissue changes following double-jaw surgery
Abstract
Purpose: It is clinically important to accurately predict facial soft-tissue changes prior to orthognathic surgery. However, the current simulation methods are problematic, especially in anatomic regions of clinical significance, e.g., the nose, lips, and chin. We developed a new 3-stage finite element method (FEM) approach that incorporates realistic tissue sliding to improve such prediction.
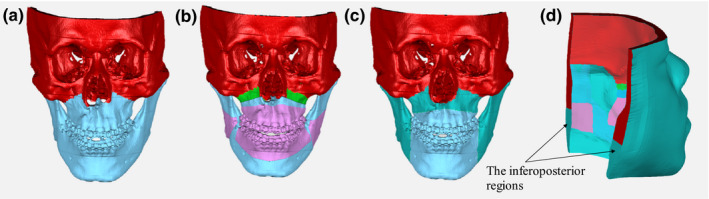
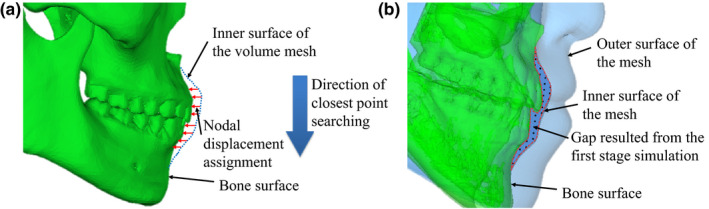
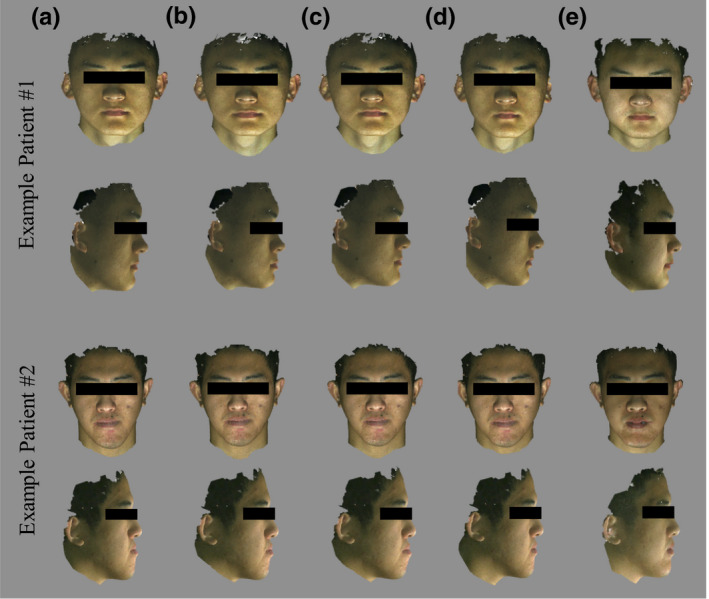
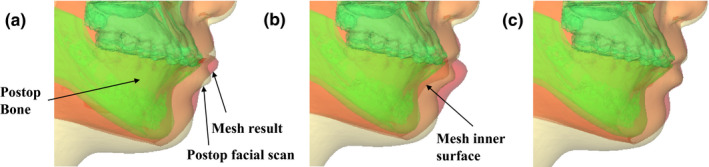
Methods: In Stage One, soft-tissue change was simulated, using FEM with patient-specific mesh models generated from our previously developed eFace template. Postoperative bone movement was applied on the patient mesh model with standard FEM boundary conditions. In Stage Two, the simulation was improved by implementing sliding effects between gum tissue and teeth using a nodal force constraint scheme. In Stage Three, the result of the tissue sliding effect was further enhanced by reassigning the soft-tissue-bone mapping and boundary conditions using nodal spatial constraint. Finally, our methods have been quantitatively and qualitatively validated using 40 retrospectively evaluated patient cases by comparing it to the traditional FEM method and the FEM with sliding effect, using a nodal force constraint method.
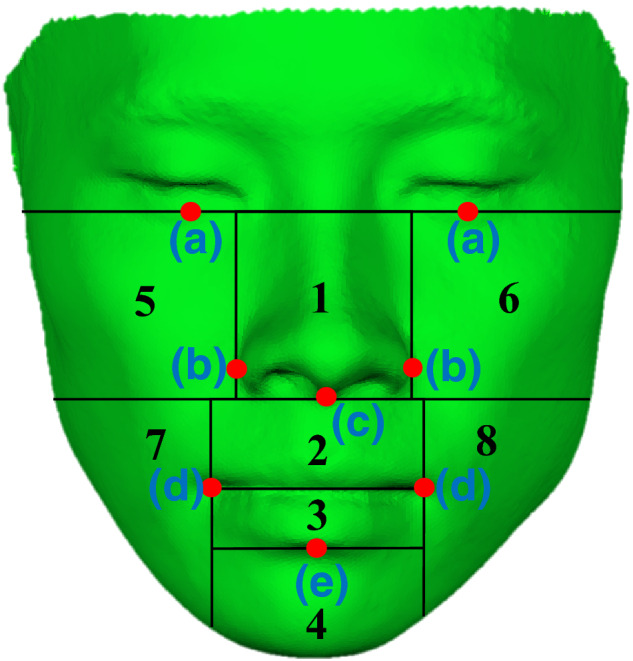
Results: The results showed that our method was better than the other two methods. Using our method, the quantitative distance errors between predicted and actual patient surfaces for the entire face and any subregions thereof were below 1.5 mm. The overall soft-tissue change prediction was accurate to within 1.1 ± 0.3 mm, with the accuracy around the upper and lower lip regions of 1.2 ± 0.7 mm and 1.5 ± 0.7 mm, respectively. The results of qualitative evaluation completed by clinical experts showed an improvement of 46% in acceptance rate compared to the traditional FEM simulation. More than 80% of the result of our approach was considered acceptable in comparison with 55% and 50% following the other two methods.
Conclusion: The FEM simulation method with improved sliding effect showed significant accuracy improvement in the whole face and the clinically significant regions (i.e., nose and lips) in comparison with the other published FEM methods, with or without sliding effect using a nodal force constraint. The qualitative validation also proved the clinical feasibility of the developed approach.
Keywords: facial soft-tissue change prediction; finite element model; orthognathic surgery; soft-tissue modeling; soft-tissue sliding effect.
© 2017 American Association of Physicists in Medicine.
Conflict of interest statement
The authors have no COI to report.
Figures
References
-
- McCormick SU, Drew SJ. Virtual model surgery for efficient planning and surgical performance. J Oral Maxillofac Surg. 2011;69:638–644. - PubMed
-
- Bobek S, Farrell B, Choi C, Farrell B, Weimer K, Tucker M. Virtual surgical planning for orthognathic surgery using digital data transfer and an intraoral fiducial marker: the charlotte method. J Oral Maxillofac Surg. 2015;73:1143–1158. - PubMed
-
- Bell WH. Modern Practice in Orthognathic and Reconstructive Surgery: volume 3. Philadelphia, PA: W.B. Saunders company; 1993.
-
- Chabanas M, Luboz V, Payan Y. Patient specific finite element model of the face soft tissues for computer‐assisted maxillofacial surgery. Med Image Anal. 2003;7:131–151. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
