

β-Blockers and Mortality After Acute Myocardial Infarction in Patients Without Heart Failure or Ventricular Dysfunction
- PMID: 28571635
- PMCID: PMC5457288
- DOI: 10.1016/j.jacc.2017.03.578
β-Blockers and Mortality After Acute Myocardial Infarction in Patients Without Heart Failure or Ventricular Dysfunction
Abstract
Background: For acute myocardial infarction (AMI) without heart failure (HF), it is unclear if β-blockers are associated with reduced mortality.
Objectives: The goal of this study was to determine the association between β-blocker use and mortality in patients with AMI without HF or left ventricular systolic dysfunction (LVSD).
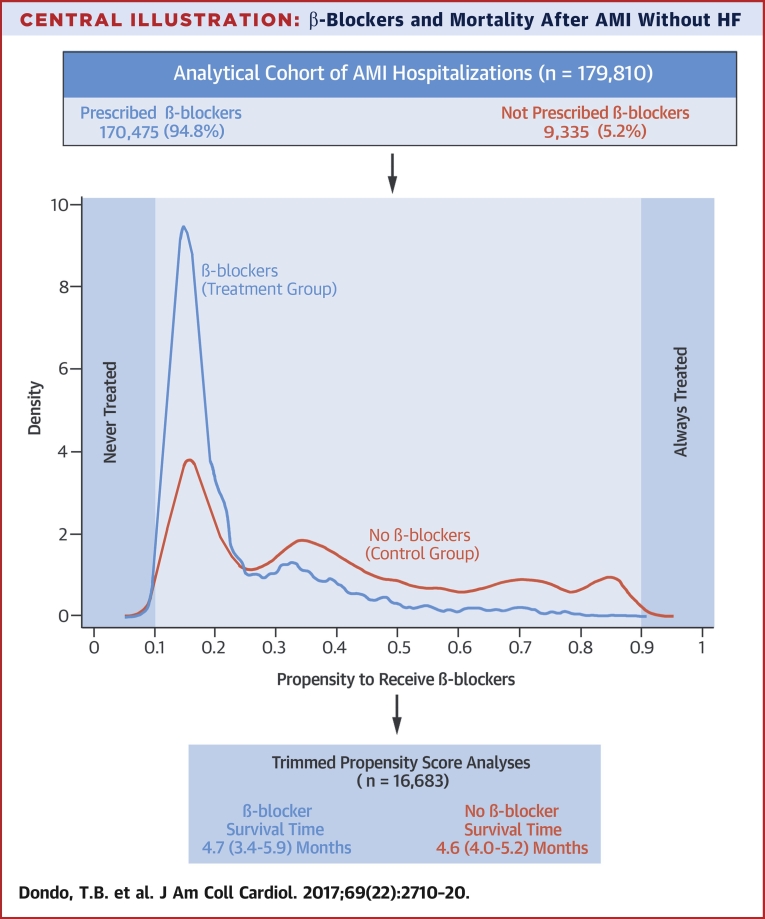
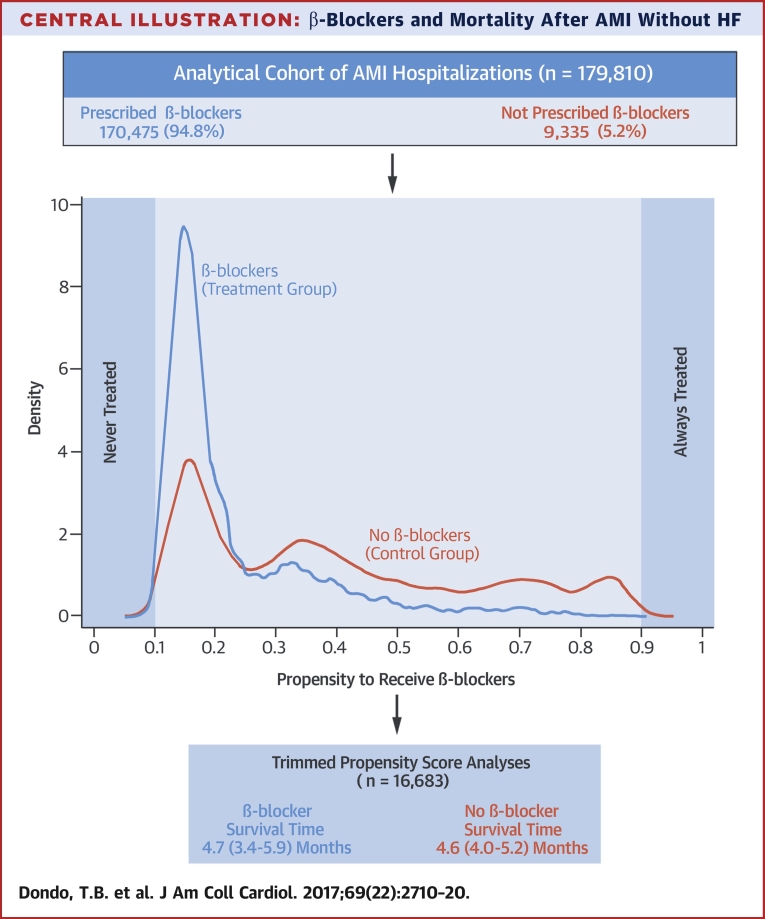
Methods: This cohort study used national English and Welsh registry data from the Myocardial Ischaemia National Audit Project. A total of 179,810 survivors of hospitalization with AMI without HF or LVSD, between January 1, 2007, and June 30, 2013 (final follow-up: December 31, 2013), were assessed. Survival-time inverse probability weighting propensity scores and instrumental variable analyses were used to investigate the association between the use of β-blockers and 1-year mortality.
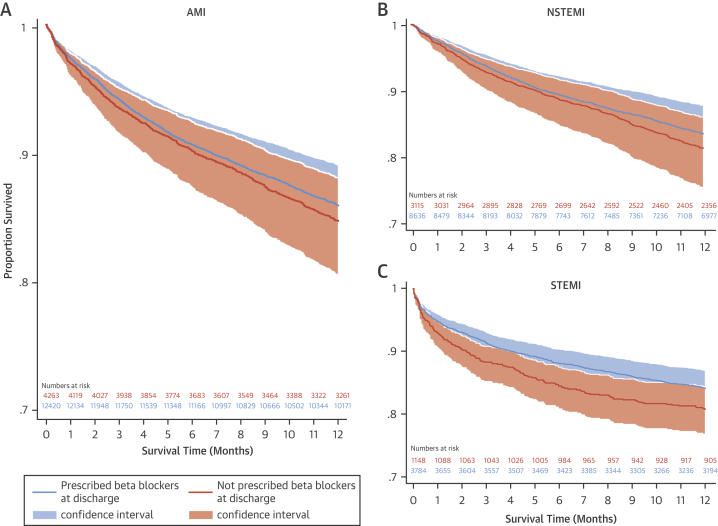
Results: Of 91,895 patients with ST-segment elevation myocardial infarction and 87,915 patients with non-ST-segment elevation myocardial infarction, 88,542 (96.4%) and 81,933 (93.2%) received β-blockers, respectively. For the entire cohort, with >163,772 person-years of observation, there were 9,373 deaths (5.2%). Unadjusted 1-year mortality was lower for patients who received β-blockers compared with those who did not (4.9% vs. 11.2%; p < 0.001). However, after weighting and adjustment, there was no significant difference in mortality between those with and without β-blocker use (average treatment effect [ATE] coefficient: 0.07; 95% confidence interval [CI]: -0.60 to 0.75; p = 0.827). Findings were similar for ST-segment elevation myocardial infarction (ATE coefficient: 0.30; 95% CI: -0.98 to 1.58; p = 0.637) and non-ST-segment elevation myocardial infarction (ATE coefficient: -0.07; 95% CI: -0.68 to 0.54; p = 0.819).
Conclusions: Among survivors of hospitalization with AMI who did not have HF or LVSD as recorded in the hospital, the use of β-blockers was not associated with a lower risk of death at any time point up to 1 year. (β-Blocker Use and Mortality in Hospital Survivors of Acute Myocardial Infarction Without Heart Failure; NCT02786654).
Keywords: NSTEMI; STEMI; average treatment effect; preserved left ventricular systolic function; propensity score; survival.
Copyright © 2017 The Authors. Published by Elsevier Inc. All rights reserved.
Figures

Comment in
-
The Swing of β-Blockers: Time for a System Reboot.J Am Coll Cardiol. 2017 Jun 6;69(22):2721-2724. doi: 10.1016/j.jacc.2017.04.017. J Am Coll Cardiol. 2017. PMID: 28571636 No abstract available.
-
Should Beta-Blockers Be Routinely Prescribed for Myocardial Infarction Without Heart Failure or Ventricular Dysfunction?J Am Coll Cardiol. 2017 Sep 26;70(13):1685-1686. doi: 10.1016/j.jacc.2017.07.760. J Am Coll Cardiol. 2017. PMID: 28935047 No abstract available.
-
β-Blockers and Outcome After Acute Myocardial Infarction.J Am Coll Cardiol. 2017 Sep 26;70(13):1685. doi: 10.1016/j.jacc.2017.06.072. J Am Coll Cardiol. 2017. PMID: 28935048 No abstract available.
-
Are beta blockers still necessary for all survivors of acute myocardial infarction?J Thorac Dis. 2017 Oct;9(10):3616-3619. doi: 10.21037/jtd.2017.09.93. J Thorac Dis. 2017. PMID: 29268356 Free PMC article. No abstract available.
-
Routine beta-blocker administration following acute myocardial infarction: why still an unsolved issue?J Thorac Dis. 2017 Nov;9(11):4191-4194. doi: 10.21037/jtd.2017.10.25. J Thorac Dis. 2017. PMID: 29268468 Free PMC article. No abstract available.
References
-
- Capricorn Investigators Effect of carvedilol on outcome after myocardial infarction in patients with left-ventricular dysfunction: the CAPRICORN randomised trial. Lancet. 2001;357:1385–1390. - PubMed
-
- Timolol-induced reduction in mortality and reinfarction in patients surviving acute myocardial infarction. N Engl J Med. 1981;304:801–807. - PubMed
-
- Yusuf S., Wittes J., Friedman L. Overview of results of randomized clinical trials in heart disease: I. Treatments following myocardial infarction. JAMA. 1988;260:2088–2093. - PubMed
-
- Chen Z., Pan H., Chen Y. Early intravenous then oral metoprolol in 45,852 patients with acute myocardial infarction: randomised placebo-controlled trial. Lancet. 2005;366:1622–1632. - PubMed
-
- Roffi M., Patrono C., Collet J.P. 2015 ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC) Eur Heart J. 2016;37:267–315. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
