

Ductular and proliferative response of esophageal submucosal glands in a porcine model of esophageal injury and repair
- PMID: 28572084
- PMCID: PMC5625137
- DOI: 10.1152/ajpgi.00036.2017
Ductular and proliferative response of esophageal submucosal glands in a porcine model of esophageal injury and repair
Abstract
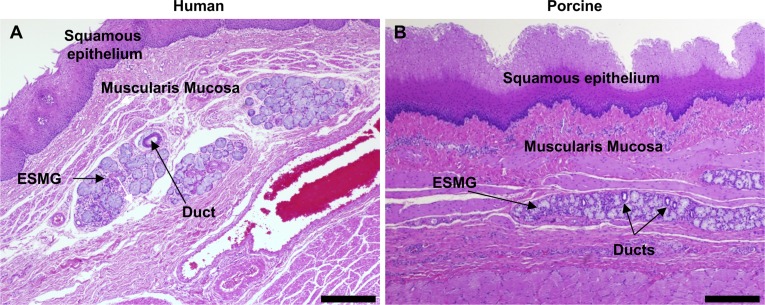
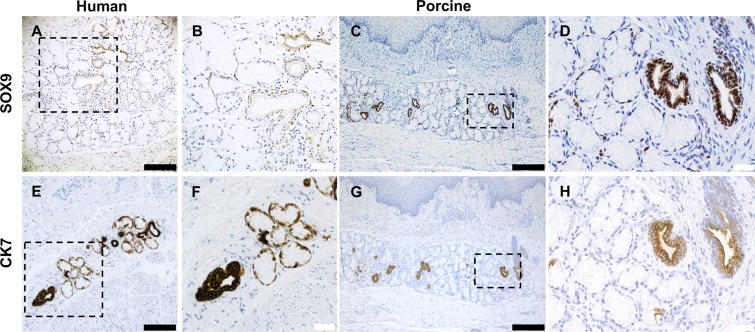
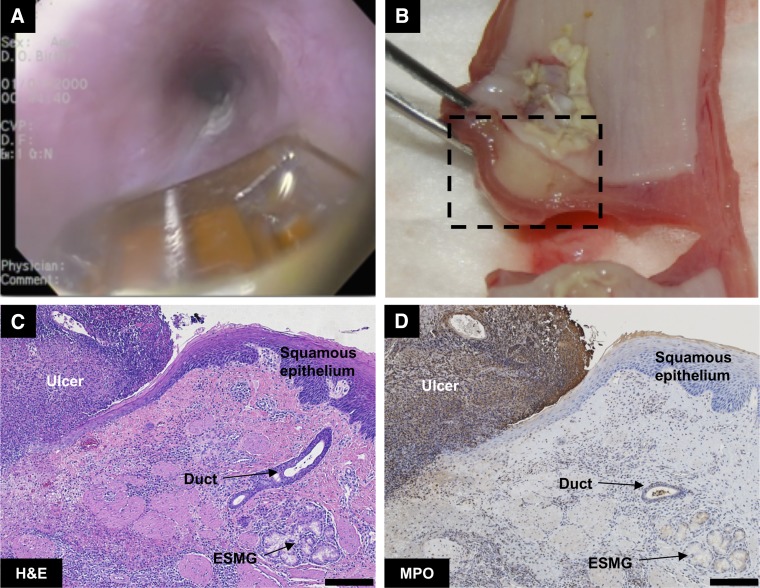
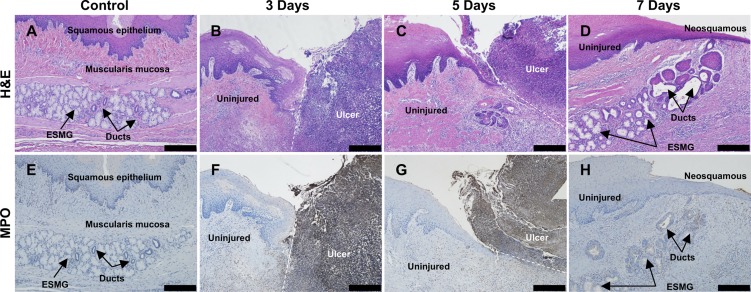
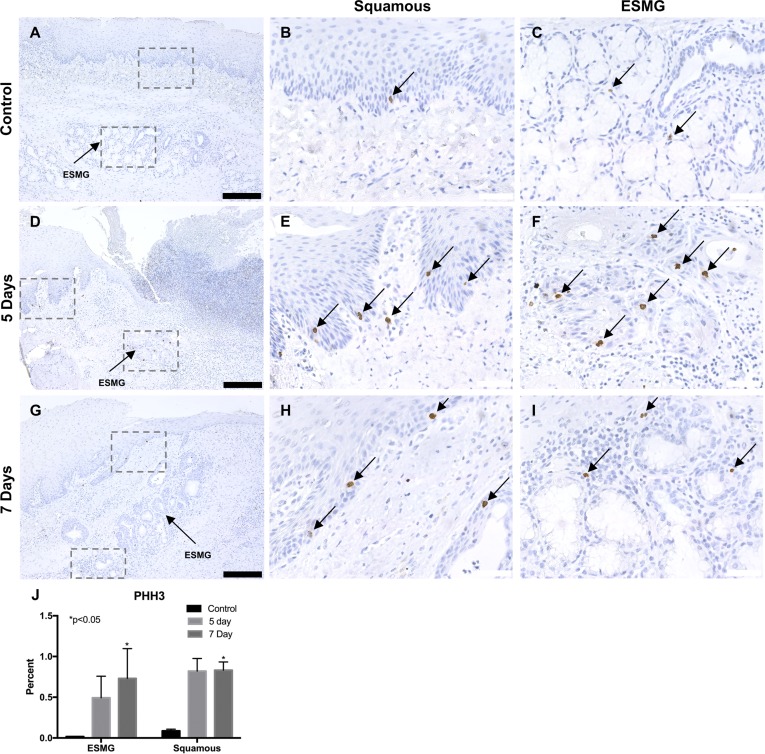
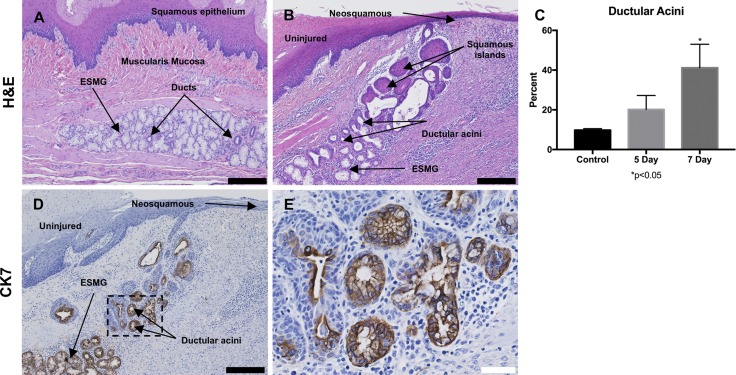
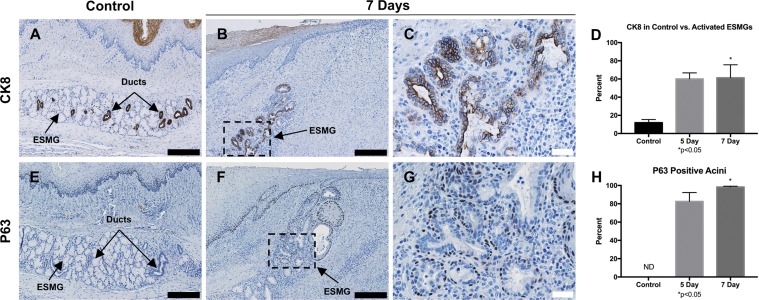
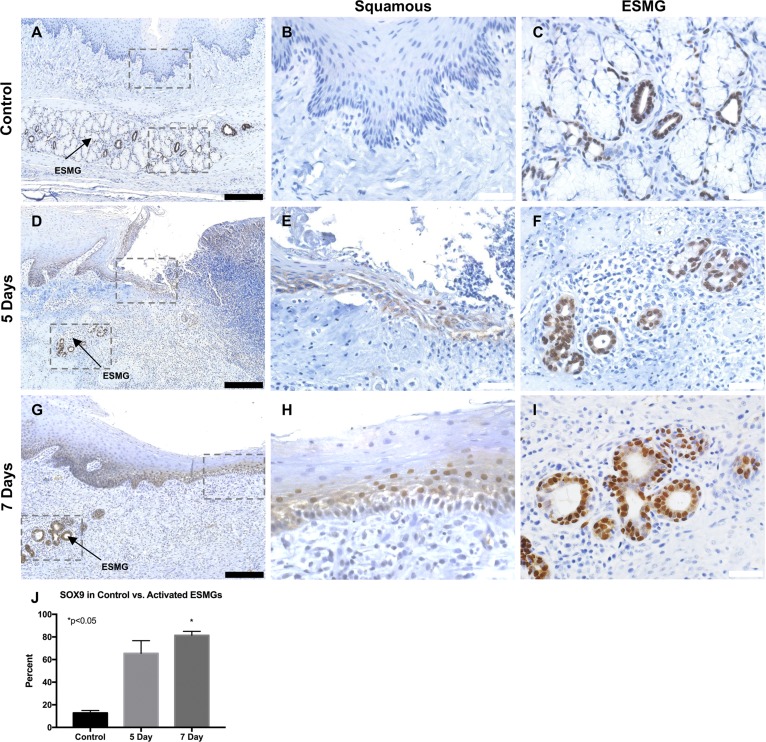
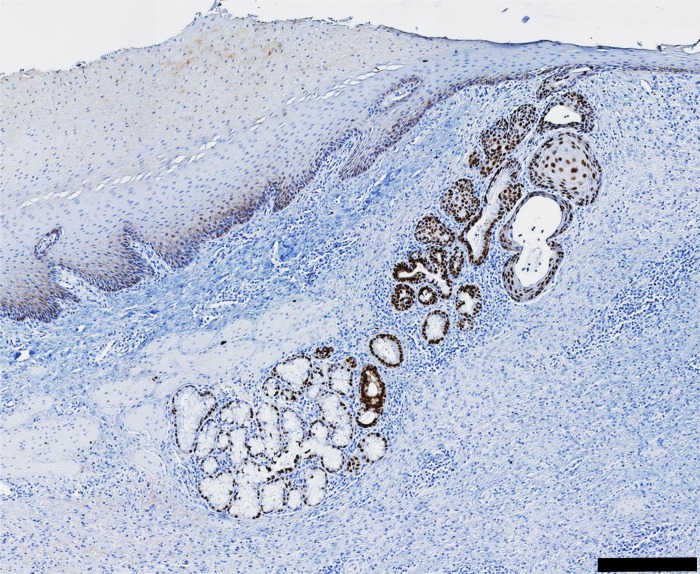
Esophageal injury is a risk factor for diseases such as Barrett's esophagus (BE) and esophageal adenocarcinoma. To improve understanding of signaling pathways associated with both normal and abnormal repair, animal models are needed. Traditional rodent models of esophageal repair are limited by the absence of esophageal submucosal glands (ESMGs), which are present in the human esophagus. Previously, we identified acinar ductal metaplasia in human ESMGs in association with both esophageal injury and cancer. In addition, the SOX9 transcription factor has been associated with generation of columnar epithelium and the pathogenesis of BE and is present in ESMGs. To test our hypothesis that ESMGs activate after esophageal injury with an increase in proliferation, generation of a ductal phenotype, and expression of SOX9, we developed a porcine model of esophageal injury and repair using radiofrequency ablation (RFA). The porcine esophagus contains ESMGs, and RFA produces a consistent and reproducible mucosal injury in the esophagus. Here we present a temporal assessment of this model of esophageal repair. Porcine esophagus was evaluated at 0, 6, 18, 24, 48, and 72 h and 5 and 7 days following RFA and compared with control uninjured esophagus. Following RFA, ESMGs demonstrated an increase in ductal phenotype, echoing our prior studies in humans. Proliferation increased in both squamous epithelium and ESMGs postinjury with a prominent population of SOX9-positive cells in ESMGs postinjury. This model promises to be useful in future experiments evaluating mechanisms of esophageal repair.NEW & NOTEWORTHY A novel porcine model of injury and repair using radiofrequency ablation has been developed, allowing for reproducible injury to the esophagus to study repair in an animal model with esophageal submucosal glands, a key anatomical feature and missing in rodent models but possibly harboring progenitor cells. There is a strong translational component to this porcine model given the anatomical and physiological similarities between pigs and humans.
Keywords: esophageal submucosal gland; esophagus; injury; proliferation; repair.
Copyright © 2017 the American Physiological Society.
Figures
References
-
- Boult J, Roberts K, Brookes MJ, Hughes S, Bury JP, Cross SS, Anderson GJ, Spychal R, Iqbal T, Tselepis C. Overexpression of cellular iron import proteins is associated with malignant progression of esophageal adenocarcinoma. Clin Cancer Res 14: 379–387, 2008. doi: 10.1158/1078-0432.CCR-07-1054. - DOI - PubMed
-
- Chen NM, Singh G, Koenig A, Liou GY, Storz P, Zhang JS, Regul L, Nagarajan S, Kühnemuth B, Johnsen SA, Hebrok M, Siveke J, Billadeau DD, Ellenrieder V, Hessmann E. NFATc1 links EGFR signaling to induction of Sox9 transcription and acinar-ductal transdifferentiation in the pancreas. Gastroenterology 148: 1024–1034.e9, 2015. doi: 10.1053/j.gastro.2015.01.033. - DOI - PMC - PubMed
-
- Clemons NJ, Wang DH, Croagh D, Tikoo A, Fennell CM, Murone C, Scott AM, Watkins DN, Phillips WA. Sox9 drives columnar differentiation of esophageal squamous epithelium: a possible role in the pathogenesis of Barrett’s esophagus. Am J Physiol Gastrointest Liver Physiol 303: G1335–G1346, 2012. doi: 10.1152/ajpgi.00291.2012. - DOI - PubMed
-
- Coad RA, Woodman AC, Warner PJ, Barr H, Wright NA, Shepherd NA. On the histogenesis of Barrett’s oesophagus and its associated squamous islands: a three-dimensional study of their morphological relationship with native oesophageal gland ducts. J Pathol 206: 388–394, 2005. doi: 10.1002/path.1804. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials