

Percutaneous Spinal Ablation in a Sheep Model: Protective Capacity of an Intact Cortex, Correlation of Ablation Parameters with Ablation Zone Size, and Correlation of Postablation MRI and Pathologic Findings
- PMID: 28572150
- PMCID: PMC7960423
- DOI: 10.3174/ajnr.A5228
Percutaneous Spinal Ablation in a Sheep Model: Protective Capacity of an Intact Cortex, Correlation of Ablation Parameters with Ablation Zone Size, and Correlation of Postablation MRI and Pathologic Findings
Abstract
Background and purpose: Despite the growing use of percutaneous ablation therapy for the treatment of metastatic spine disease, several issues have yet to be fully addressed. Our aims were to determine whether the vertebral body cortex protects against ablation-induced spinal cord injury; correlate radiofrequency, cryo-, and microwave ablation parameters with resulting spinal ablation zone dimensions and describe normal spinal marrow postablation changes on MR imaging.
Materials and methods: Ten thoracolumbar vertebrae in 3 sheep were treated with radiofrequency ablation, cryoablation, or microwave ablation under fluoroscopic guidance. Technique parameters were chosen to produce ablation zones that exceeded the volume of the vertebral bodies in sheep 1 and were confined to the vertebrae in sheep 2 and 3. Expected ablation zone dimensions were based on data provided by the device manufacturers. Postablation MR imaging was performed at 48 hours (sheep 1) or 7 days (sheep 2 and 3).
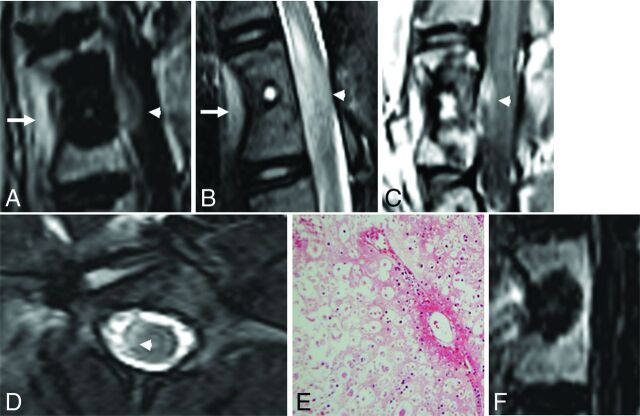
Results: In sheep 1, cryoablation and microwave ablations extended into the spinal canal and caused histologically confirmed neurologic injury, but radiofrequency ablation did not. The mean difference between the lengths of the radiofrequency ablation zone dimensions measured on gross pathology compared with those expected was 9.6 ± 4.1 mm. The gross pathologic cryo- and microwave ablation zone dimensions were within 1 mm of those expected. All modalities produced a nonenhancing ablation zone with a rim of enhancement, corresponding histologically to marrow necrosis and hemorrhagic congestion.
Conclusions: An intact cortex appears to protect against radiofrequency ablation-induced spinal cord injury, but not against non-impedance-based modalities. Ablation dimensions produced by microwave and cryoablation are similar to those expected, while radiofrequency ablation dimensions are smaller. Ablation of normal marrow produces a rim of enhancement at the margin of the ablation zone on MR imaging.
© 2017 by American Journal of Neuroradiology.
Figures




Comment in
-
Is an Intact Posterior Vertebral Body Cortex Protective for Percutaneous Ablation?AJNR Am J Neuroradiol. 2017 Aug;38(8):1660-1661. doi: 10.3174/ajnr.A5235. Epub 2017 Jun 1. AJNR Am J Neuroradiol. 2017. PMID: 28572151 Free PMC article. No abstract available.
-
Bipolar Radiofrequency Ablation of Spinal Tumors: The Effect of the Posterior Vertebral Cortex Defect on Temperature Distribution in the Spinal Canal.AJNR Am J Neuroradiol. 2018 Jan;39(1):E1-E2. doi: 10.3174/ajnr.A5393. Epub 2017 Nov 16. AJNR Am J Neuroradiol. 2018. PMID: 29146717 Free PMC article. No abstract available.
References
-
- Anchala PR, Irving WD, Hillen TJ, et al. . Treatment of metastatic spinal lesions with a navigational bipolar radiofrequency ablation device: a multicenter retrospective study. Pain Physician 2014;17:317–27 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources