

Shared decision-making for biologic treatment of autoimmune disease: influence on adherence, persistence, satisfaction, and health care costs
- PMID: 28572722
- PMCID: PMC5441672
- DOI: 10.2147/PPA.S133222
Shared decision-making for biologic treatment of autoimmune disease: influence on adherence, persistence, satisfaction, and health care costs
Abstract
Background: Shared decision-making (SDM), a process whereby physicians and patients collaborate to select interventions, is not well understood for biologic treatment of autoimmune conditions.
Methods: This was a cross-sectional survey of adults initiating treatment for Crohn's disease or ulcerative colitis (inflammatory bowel disease, IBD) or psoriatic arthritis or rheumatoid arthritis (RA/PA). Survey data were linked to administrative claims for 6 months before (baseline) and after (follow-up) therapy initiation. Measures included the Shared Decision Making Questionnaire, Patient Activation Measure (PAM), Morisky Medication Adherence Scale (MMAS), general health, and treatment satisfaction. Claims-based Quan-Charlson comorbidity scores, persistence, medication possession ratio (MPR), and health care costs were examined. Patients were compared by participation (SDM) and nonparticipation (non-SDM) in SDM.
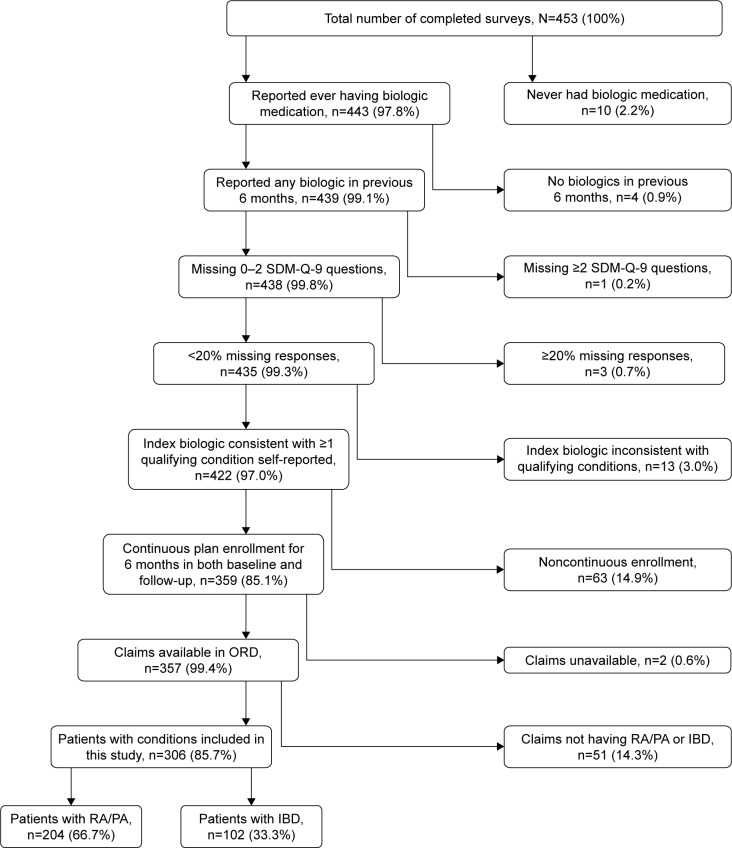
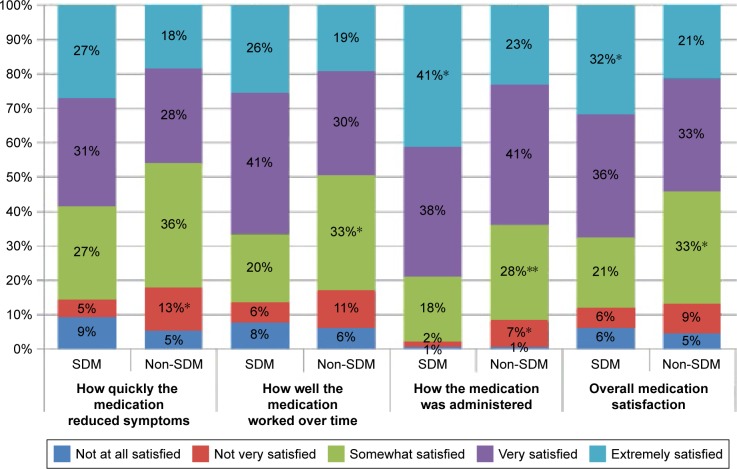
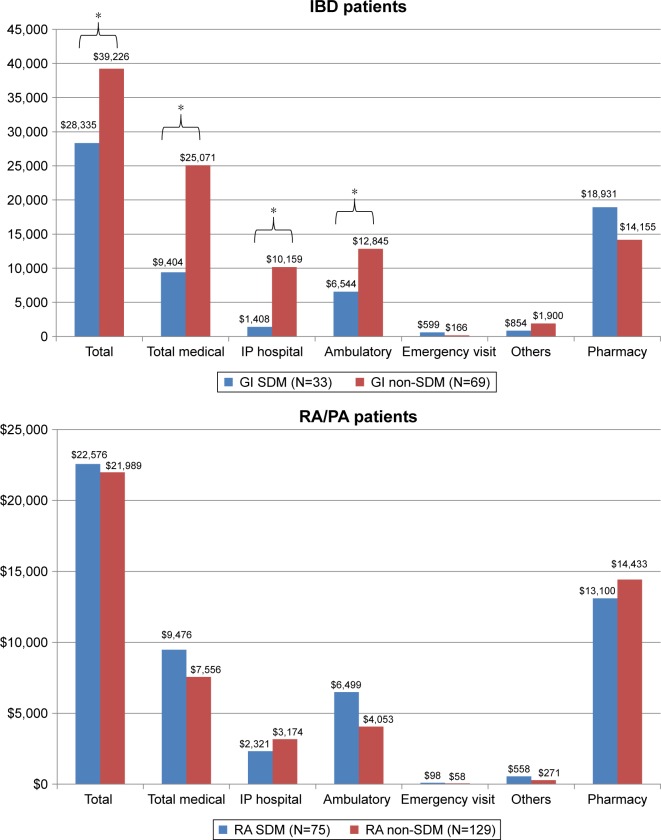
Results: Among 453 respondents, 357 were eligible, and 306 patients (204 RA/PA and 102 IBD) were included in all analyses. Overall (n=357), SDM participants (n=120) were more often females (75.0% vs 62.5%, P=0.018), had lower health status (48.0 vs 55.4, P=0.005), and higher Quan-Charlson scores (1.0 vs 0.7, P=0.035) than non-SDM (n=237) participants. Lower MMAS scores (SDM 0.17 vs non-SDM 0.41; P<0.05) indicated greater likelihood of adherence; SDM participants also reported higher satisfaction with medication and had greater activation (PAM: SDM vs non-SDM: 66.9 vs 61.6; P<0.001). Mean MPR did not differ, but persistence was longer among SDM participants (111.2 days vs 102.2 days for non-SDM; P=0.029). Costs did not differ by SDM status overall, or among patients with RA/PA. The patients with IBD, however, experienced lower (P=0.003) total costs ($9,404 for SDM vs $25,071 for non-SDM) during follow-up.
Conclusion: This study showed greater likelihood of adherence and satisfaction for patients who engaged in SDM and reduced health care costs among patients with IBD who engaged in SDM. This study provides a basis for defining SDM participation and detecting differences by SDM participation for biologic treatment selection for autoimmune conditions.
Keywords: autoimmune disease; biologic therapy; cross-sectional survey; shared decisionmaking.
Conflict of interest statement
Disclosure At the time of the study, JHL, MPI, and LE were employees of Janssen Scientific Affairs, LLC, and stockholders in Johnson & Johnson. PTJ, JCW, and SCR were employees of Optum Inc., and were funded by Janssen Scientific Affairs, LLC, to conduct the study. Their employment was not contingent upon this funding. The authors report no other conflicts of interest in this work.
Figures
References
-
- Shafir A, Rosenthal J. Shared Decision Making: Advancing Patient-Centered Care through State and Federal Implementation. Washington, DC: National Academy for State Health Policy; 2012. [Accessed January 24, 2017]. Available from: http://www.nashp.org/sites/default/files/shared.decision.making.report.pdf.
-
- Department of Health and Human Services . National Strategy for Quality Improvement in Health Care: Agency-specific Quality Strategic Plans. Bethesda, MD: DHHS; 2011. [Accessed January 24, 2017]. Available from: https://www.ahrq.gov/workingforquality/nqs/nqsplans.pdf.
-
- Elwyn G, Lloyd A, May C, et al. Collaborative deliberation: a model for patient care. Patient Educ Couns. 2014;97(2):158–164. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
