

Inertial Sensors to Assess Gait Quality in Patients with Neurological Disorders: A Systematic Review of Technical and Analytical Challenges
- PMID: 28572784
- PMCID: PMC5435996
- DOI: 10.3389/fpsyg.2017.00817
Inertial Sensors to Assess Gait Quality in Patients with Neurological Disorders: A Systematic Review of Technical and Analytical Challenges
Abstract
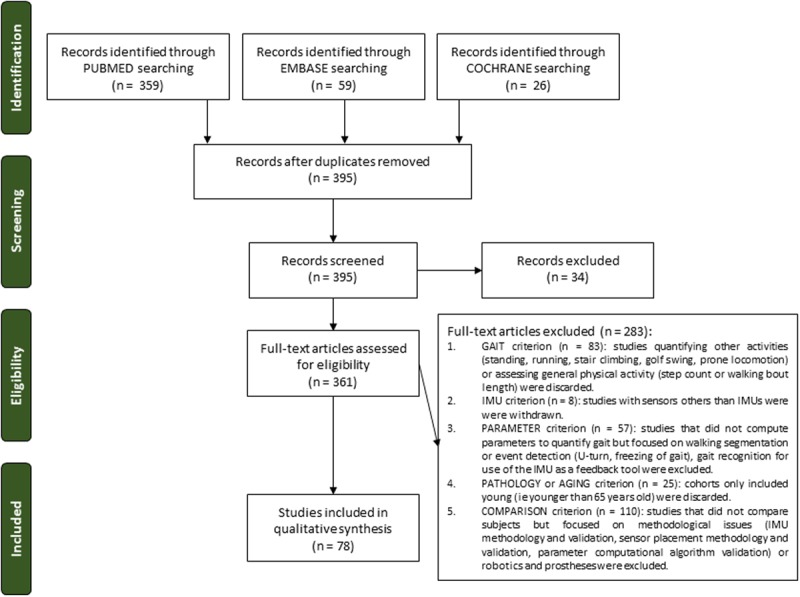
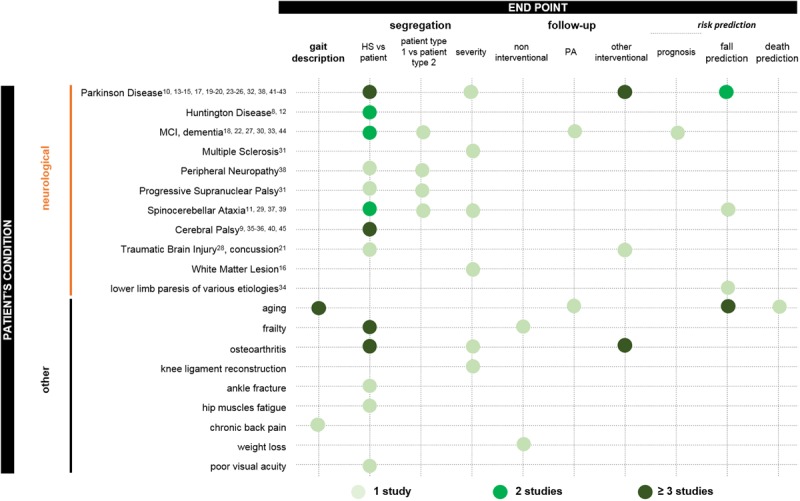
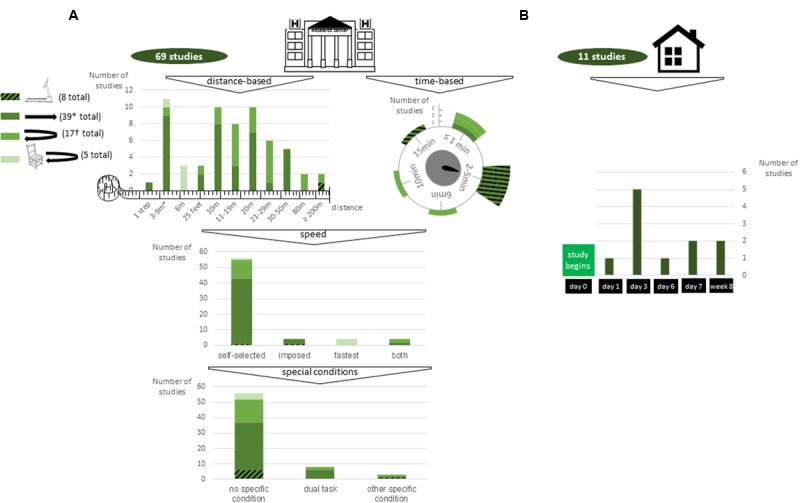
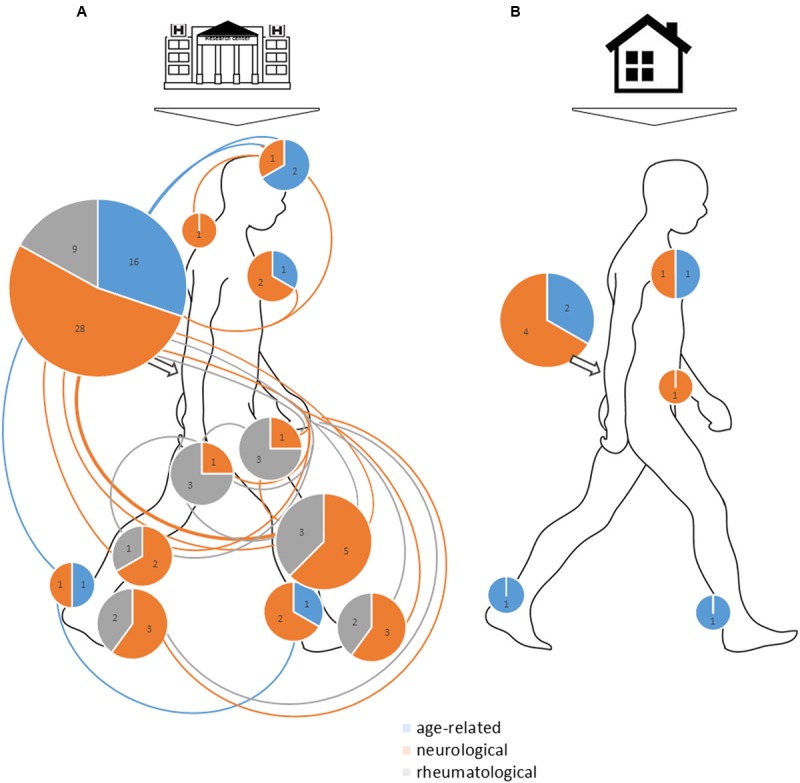
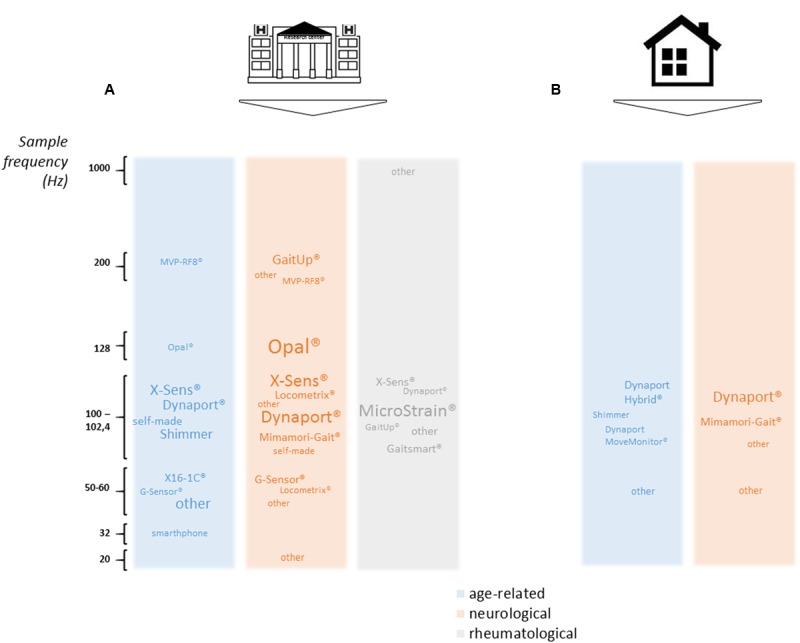
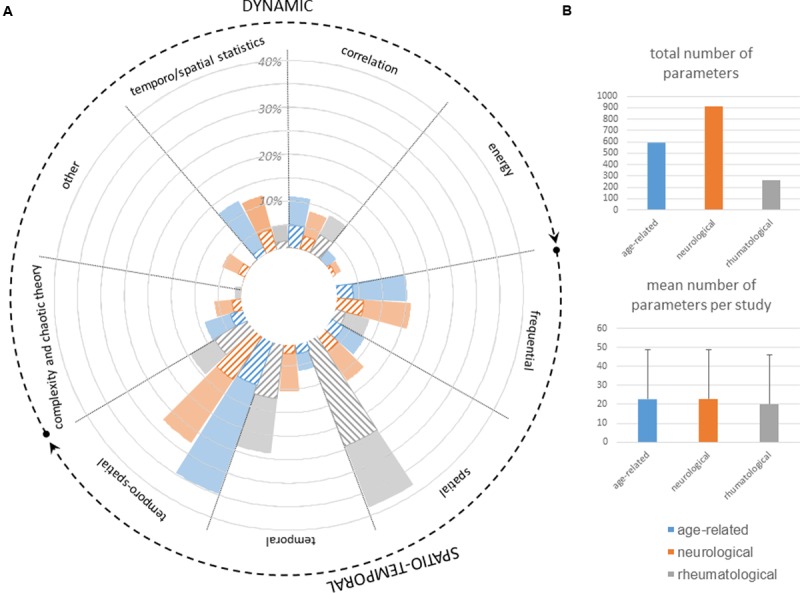
Gait disorders are major causes of falls in patients with neurological diseases. Understanding these disorders allows prevention and better insights into underlying diseases. InertiaLocoGraphy (ILG) -the quantification of gait by using inertial measurement units (IMUs) -shows great potential to address this public health challenge, but protocols vary widely and normative values of gait parameters are still unavailable. This systematic review critically compares ILG protocols, questions features extracted from inertial signals and proposes a semeiological analysis of clinimetric characteristics for use in neurological clinical routine. For this systematic review, PubMed, Cochrane and EMBASE were searched for articles assessing gait quality by using IMUs that were published from January 1, 2014 to August 31, 2016. ILG was used to assess gait in a wide range of neurological disorders - including Parkinson disease, mild cognitive impairment, Alzheimer disease, cerebral palsy, and cerebellar atrophy - as well as in the faller or frail older population and in people presenting rheumatological pathologies. However, results have not yet been driving changes in clinical practice. One reason could be that studies mainly aimed at comparing pathological gait to healthy gait, but there is stronger need for semiological descriptions of gait perturbation, severity or prognostic assessment. Furthermore, protocols used to assess gait using IMUs are too many. Likely, outcomes are highly heterogeneous and difficult to compare across large panels of studies. Therefore, homogenization is needed to foster the use of ILG to assess gait quality in neurological routine practice. The pros and cons of each protocol are emphasized so that a compromise can be reached. As well, analysis of seven complementary clinical criteria (springiness, sturdiness, smoothness, steadiness, stability, symmetry, synchronization) is advocated.
Keywords: accelerometer; gait analysis; gait disorders; inertial measurement unit; wearable inertial sensors.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous