

The impacts of different embolization techniques on splenic artery embolization for blunt splenic injury: a systematic review and meta-analysis
- PMID: 28573044
- PMCID: PMC5450228
- DOI: 10.1186/s40779-017-0125-6
The impacts of different embolization techniques on splenic artery embolization for blunt splenic injury: a systematic review and meta-analysis
Abstract
Background: Splenic artery embolization (SAE) has been an effective adjunct to the Non-operative management (NOM) for blunt splenic injury (BSI). However, the optimal embolization techniques are still inconclusive. To further understand the roles of different embolization locations and embolic materials in SAE, we conducted this system review and meta-analyses.
Methods: Clinical studies related to SAE for adult patients were researched in electronic databases, included PubMed, Embase, ScienceDirect and Google Scholar Search (between October 1991 and March 2013), and relevant information was extracted. To eliminate the heterogeneity, a sensitivity analysis was conducted on two reduced study sets. Then, the pooled outcomes were compared and the quality assessments were performed using Newcastle-Ottawa Scale (NOS). The SAE success rate, incidences of life-threatening complications of different embolization techniques were compared by χ2 test in 1st study set. Associations between different embolization techniques and clinical outcomes were evaluated by fixed-effects model in 2nd study set.
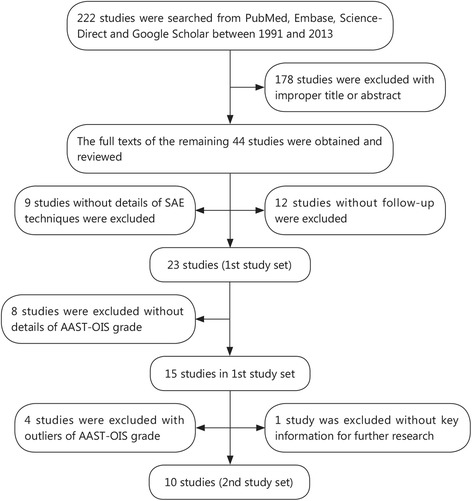
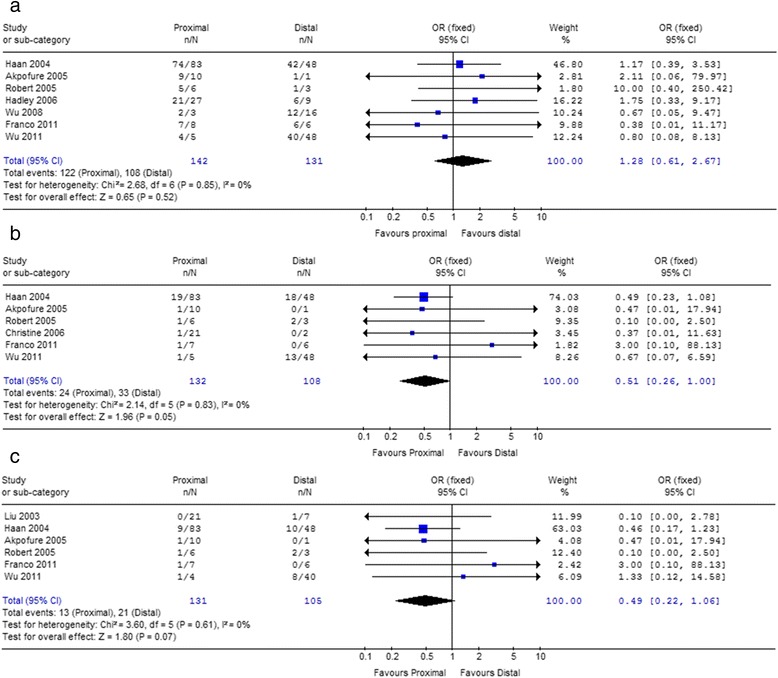
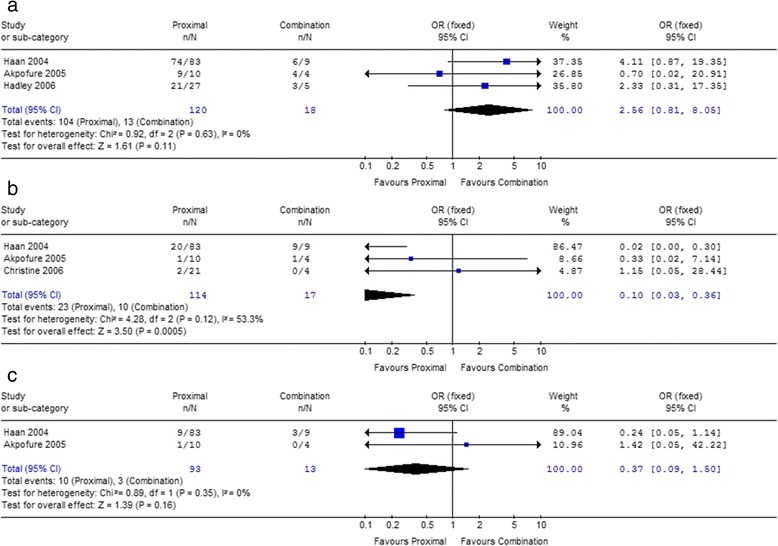
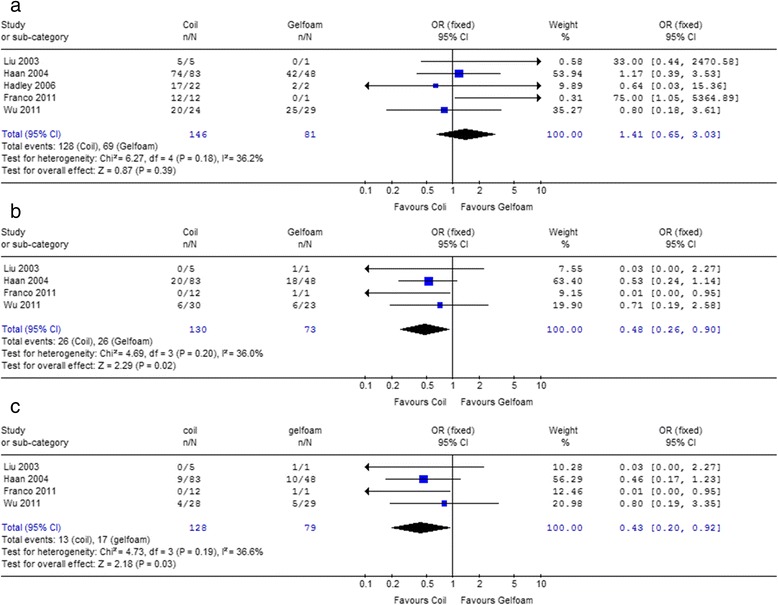
Results: Twenty-three studies were included in 1st study set. And then, 13 of them were excluded, because lack of the necessary details of SAE. The remaining 10 studies comprised 2nd study set, and quality assessments were performed using NOS. In 1st set, the primary success rate is 90.1% and the incidence of life-threatening complications is 20.4%, though the cases which required surgical intervention are very few (6.4%). For different embolization locations, there was no obvious association between primary success rate and embolization location in both 1st and 2nd study sets (P > 0.05). But in 2nd study set, it indicated that proximal embolization reduced severe complications and complications needed surgical management. As for the embolic materials, the success rate between coil and gelfoam is not significant. However, coil is associated with a lower risk of life-threatening complications, as well as less complications requiring surgical management.
Conclusions: Different embolization techniques affect the clinical outcomes of SAE. The proximal embolization is the best option due to the less life-threatening complications. For commonly embolic material, coil is superior to gelfoam for fewer severe complications and less further surgery management.
Keywords: Blunt splenic injury; Clinical outcome; Embolization; Location; Material.
Figures
Similar articles
-
The role of splenic angioembolization as an adjunct to nonoperative management of blunt splenic injuries: A systematic review and meta-analysis.J Trauma Acute Care Surg. 2017 Nov;83(5):934-943. doi: 10.1097/TA.0000000000001649. J Trauma Acute Care Surg. 2017. PMID: 29068875
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
Splenic artery embolization in the treatment of blunt splenic injury: single level 1 trauma center experience.Diagn Interv Radiol. 2025 Jul 8;31(4):359-365. doi: 10.4274/dir.2024.242789. Epub 2024 Jul 11. Diagn Interv Radiol. 2025. PMID: 38988193 Free PMC article.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of topotecan for ovarian cancer.Health Technol Assess. 2001;5(28):1-110. doi: 10.3310/hta5280. Health Technol Assess. 2001. PMID: 11701100
-
Intravenous magnesium sulphate and sotalol for prevention of atrial fibrillation after coronary artery bypass surgery: a systematic review and economic evaluation.Health Technol Assess. 2008 Jun;12(28):iii-iv, ix-95. doi: 10.3310/hta12280. Health Technol Assess. 2008. PMID: 18547499
Cited by
-
Management of Hemodynamic Collapse After Liver Transplantation From Native Bile Duct Stump Hemorrhage with Gelfoam.ACG Case Rep J. 2019 Oct 17;6(10):e00254. doi: 10.14309/crj.0000000000000254. eCollection 2019 Oct. ACG Case Rep J. 2019. PMID: 31832474 Free PMC article.
-
Splenic Artery Embolization for Patients with High-Grade Splenic Trauma: Indications, Techniques, and Clinical Outcomes.Semin Intervent Radiol. 2021 Mar;38(1):105-112. doi: 10.1055/s-0041-1724010. Epub 2021 Apr 15. Semin Intervent Radiol. 2021. PMID: 33883807 Free PMC article. Review.
-
Simultaneous CSM-TACE with CalliSpheres® and partial splenic embolization using 8spheres® for hepatocellular carcinoma with hypersplenism: Early prospective multicenter clinical outcome.Front Oncol. 2022 Dec 1;12:998500. doi: 10.3389/fonc.2022.998500. eCollection 2022. Front Oncol. 2022. PMID: 36530976 Free PMC article.
-
The predictive value of CTSI scoring system in non-operative management of patients with splenic blunt trauma: The experience of a level 1 trauma center.Eur J Radiol Open. 2023 Sep 23;11:100525. doi: 10.1016/j.ejro.2023.100525. eCollection 2023 Dec. Eur J Radiol Open. 2023. PMID: 37771658 Free PMC article.
-
Optimizing distal and proximal splenic artery embolization with patient-specific computational fluid dynamics.J Biomech. 2024 Nov;176:112320. doi: 10.1016/j.jbiomech.2024.112320. Epub 2024 Sep 12. J Biomech. 2024. PMID: 39276470
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
