

Endoscopic esophagogastric anastomosis with luminal apposition Axios stent (LAS) approach: a new concept for hybrid "Lewis Santy"
- PMID: 28573178
- PMCID: PMC5451277
- DOI: 10.1055/s-0043-106577
Endoscopic esophagogastric anastomosis with luminal apposition Axios stent (LAS) approach: a new concept for hybrid "Lewis Santy"
Erratum in
-
Erratum: Endoscopic esophagogastric anastomosis with luminal apposition Axios stent (LAS) approach: a new concept for hybrid "Lewis Santy".Endosc Int Open. 2017 Jun;5(6):C5. doi: 10.1055/s-0044-100438. Epub 2018 Jan 12. Endosc Int Open. 2017. PMID: 29340291 Free PMC article.
Abstract
Background and study aims: Esophagogastric anastomosis (EGA) has a high risk of leakage. Based upon our experience in endoscopic gastrojejunal anastomosis using LAS, the aim of this study was to verify the technical feasibility and the safety of performing an EGA using a hybrid approach (endoscopic and surgical).
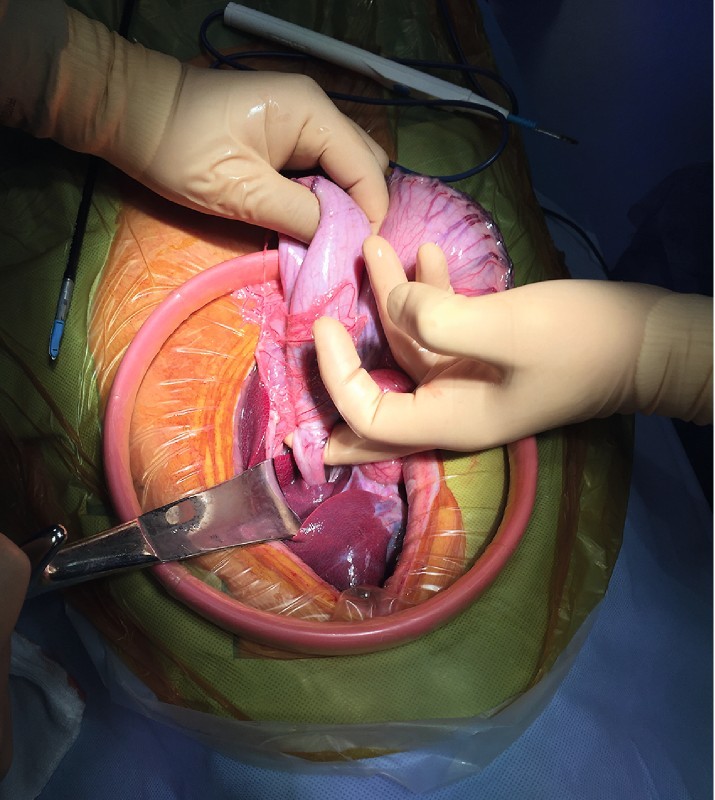
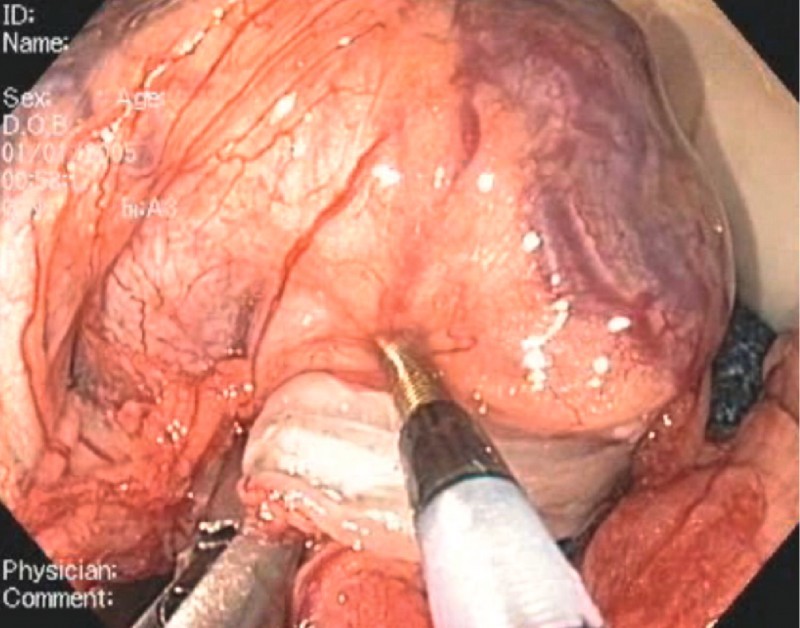
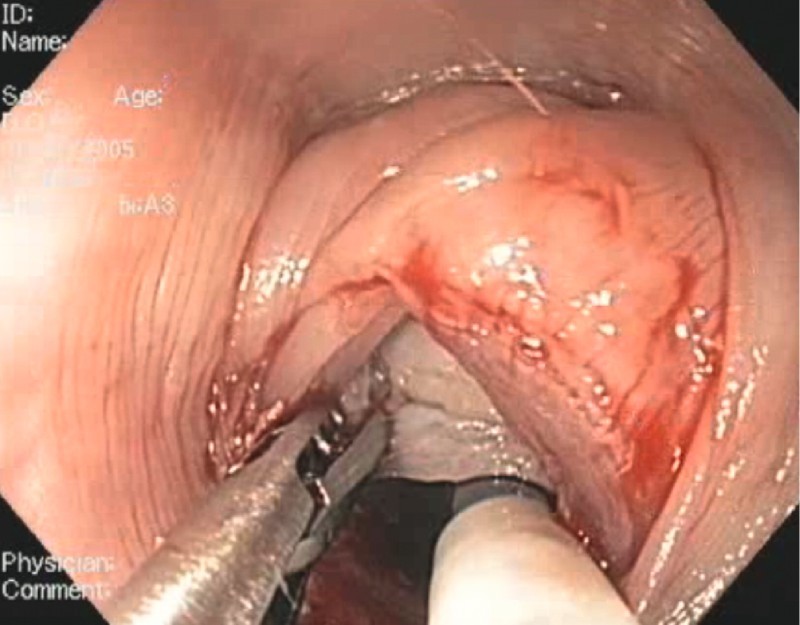
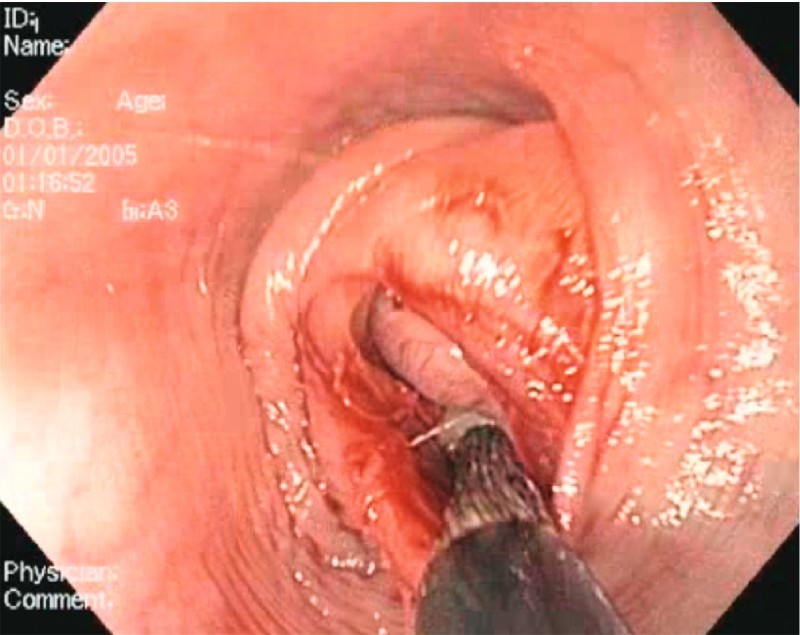
Materials and methods: A pilot prospective study was performed on 8 survival pigs. The procedure was carried out in 2 stages: (i) surgical step consisting of an esogastrectomy by laparotomy with separated suture of the esophagus and stomach; (ii) endoscopic esophagogastric anastomosis using the LAS. The first 2 pigs allowed for the setting of the 2 steps procedure, and 6 were included in the study for assessing the efficacy and safety of the procedure with a 3-week survival course. The primary endpoint was morbidity and mortality.
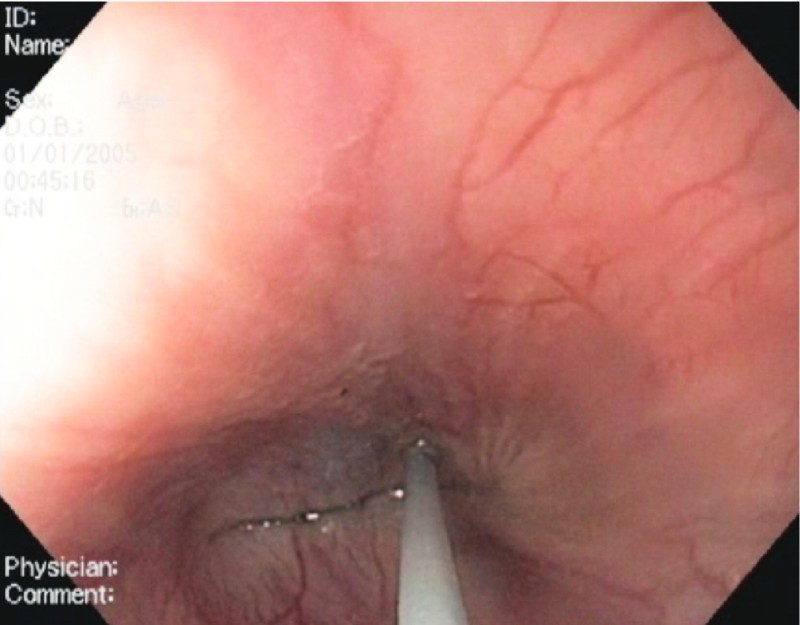
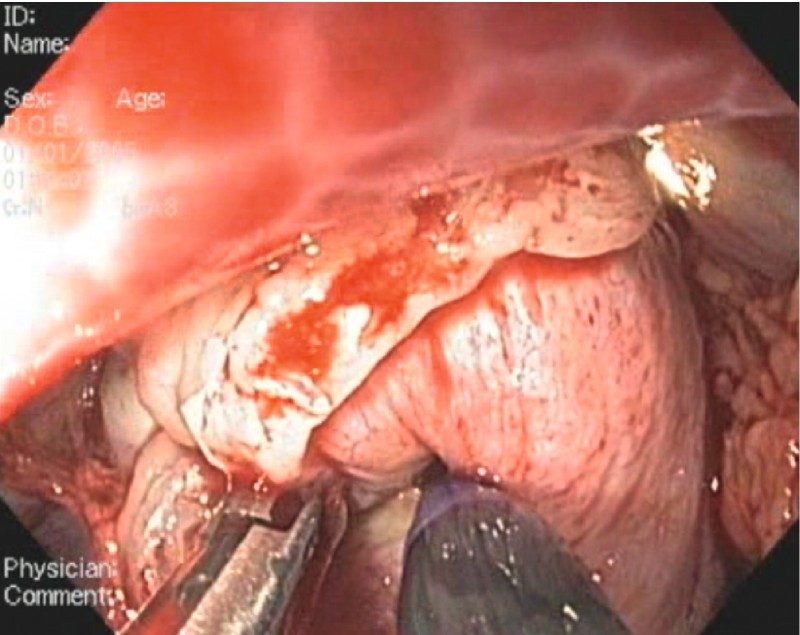
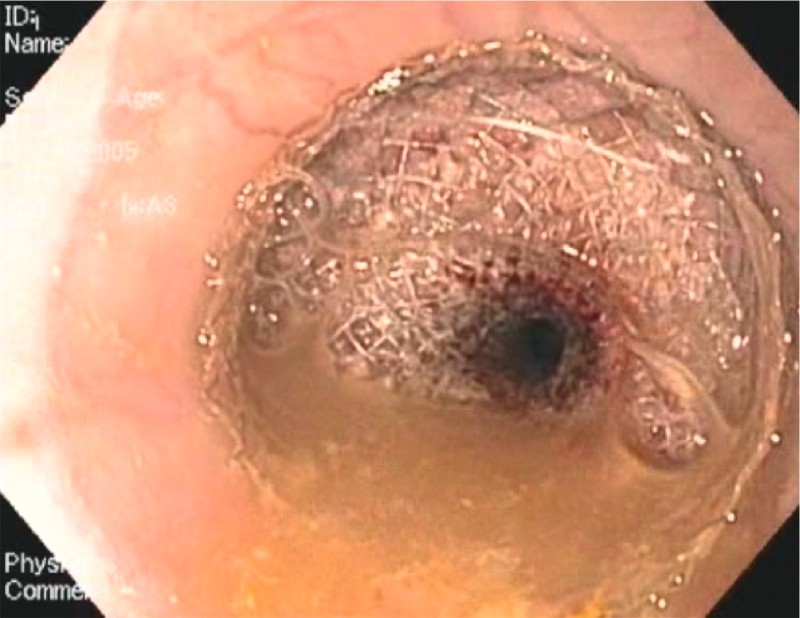
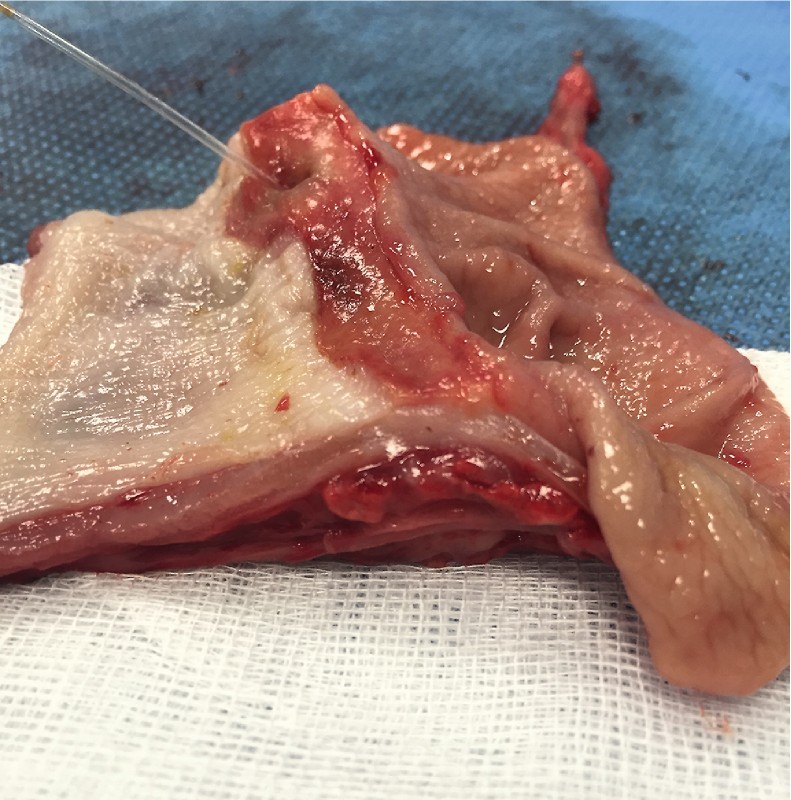
Results: All procedures were successfull. The mean operative time was 98 minutes, with a mean endoscopic time of 46 minutes. Three early deaths occurred within the first weeks, unrelated to the LAS anastomosis. At 3 weeks, endoscopic assessment followed by necropsy demonstrated the right position and the endoscopic removability of the stent with good patency of the esophagogastric anastomosis, without leakage of the endoscopic suture. Pathological examination confirmed the patency of the anastomosis with fusion of mucosal and muscle layers.
Conclusion: Endoscopic esophagogastric anastomosis with LAS is feasible and reproducible, without anastomotic leakage. It could be a new alternative to perform safe anastomoses, as part of a hybrid approach (surgical and endoscopic).
Conflict of interest statement
Figures
References
-
- Mariette C, Triboulet J P. [Complications following oesophagectomy: mechanism, detection, treatment and prevention] J Chir (Paris) 2005;142:348–354. - PubMed
-
- Watson D I, Davies N, Jamieson G G. Totally endoscopic Ivor Lewis esophagectomy. Surg Endosc. 1999;13:293–297. - PubMed
-
- Bailey S H, Bull D A, Harpole D Het al.Outcomes after esophagectomy: a ten-year prospective cohort Ann Thorac Surg 200375217–222.; discussion 222 - PubMed
-
- Vanbiervliet G, Bonin E A, Garcès R et al.Gastrojejunal anastomosis using a tissue-apposing stent: a safety and feasibility study in live pigs. Endoscopy. 2014;46:871–877. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources