

K time & maximum amplitude of thromboelastogram predict post-central venous cannulation bleeding in patients with cirrhosis: A pilot study
- PMID: 28574019
- PMCID: PMC5460579
- DOI: 10.4103/ijmr.IJMR_749_14
K time & maximum amplitude of thromboelastogram predict post-central venous cannulation bleeding in patients with cirrhosis: A pilot study
Abstract
Background & objectives: Coagulation and haemostasis are dynamic processes. The haemostatic changes in liver disease affect all aspects of coagulation. The prothrombin time (PT)/ international normalized ratio (INR) was developed to monitor oral anticoagulant therapy and the activated partial thromboplastin time to investigate inheritable single factor deficiencies. Viscoelastic tests such as thromboelastogram (TEG) give information about dynamics of clot formation (coagulation factor and anticoagulant activity), clot strength (platelets and fibrinogen) and clot stability (finbrinolysis and factor XIII). Administration of blood products before invasive procedures is still guided by INR and platelet count in patients of liver disease. This study was aimed to evaluate the validity of TEG to predict post-procedural bleed after central venous cannulation in patients with cirrhosis.
Methods: Ninety patients aged 20-70 yr diagnosed with liver cirrhosis requiring elective central venous catheter (CVC) insertion were studied. Platelet count, INR, serum creatinine, TEG and Child-Turcotte-Pugh (CTP) score were recorded before the procedure. Right-sided internal jugular vein was cannulated. On the basis of presence or absence of post-procedural bleed, patients were divided into bleeding and non-bleeding groups. The CTP score, component of TEG (R - reaction time, K - coagulation time, MA - maximum amplitude and α - angle) and laboratory parameters of both the groups were compared.
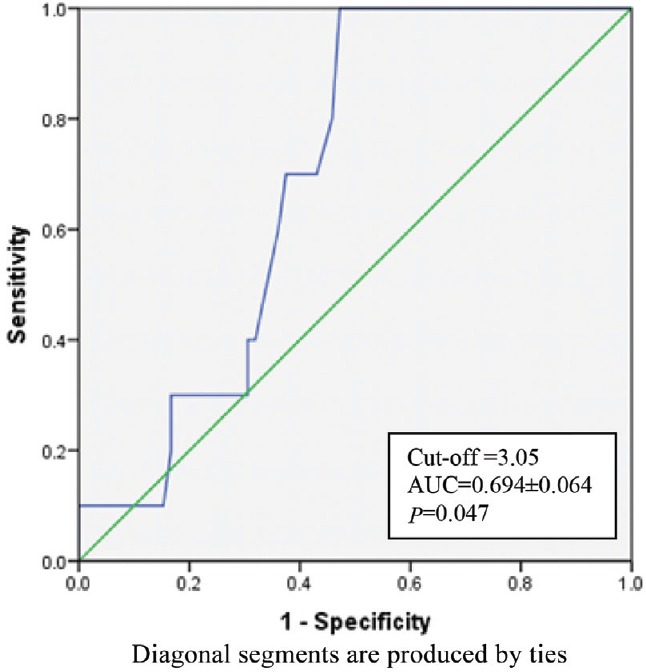
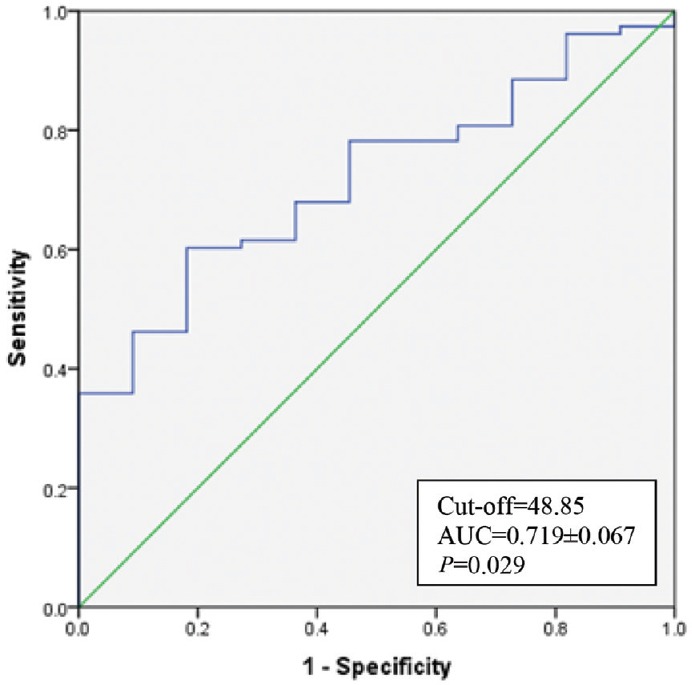
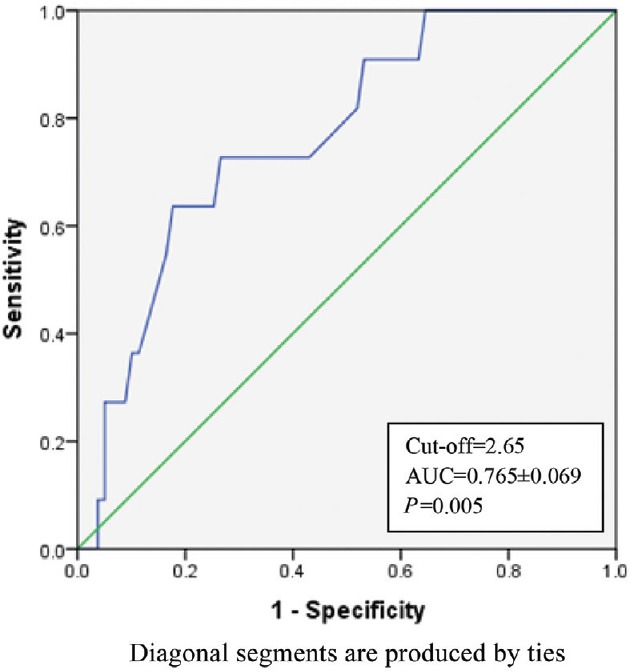
Results: Bleeding was seen more when CTP scores were ≥10 (P=0.05). The K time of 3.05 min or more on thromboelastograph was a significant predictor of bleeding [area under the curve (AUC) 0.694, P=0.047]. MA of 48.8 mm or more was a significant predictor of non-bleeding. INR ≥2.6 was a significant predictor of bleeding (AUC 0.765, P=0.005). K time had a low-positive predictive value of 20 per cent and the positive and negative likelihood ratios of 1.87 and 0.48, respectively.
Interpretation & conclusions: Our results show that the cut-off value for INR ≥2.6 and K time ≥3.05 min predict bleeding and MA ≥48.8 mm predicts non-bleeding in patients with cirrhosis undergoing central venous pressure catheter cannulation.
Conflict of interest statement
Figures
Similar articles
-
Reduced Clot Stability by Thromboelastography as a Potential Indicator of Procedure-Related Bleeding in Decompensated Cirrhosis.Hepatol Commun. 2020 Dec 12;5(2):272-282. doi: 10.1002/hep4.1641. eCollection 2021 Feb. Hepatol Commun. 2020. PMID: 33553974 Free PMC article.
-
[Application of thromboelastogram in reasonable transfusion for hospitalixed patients with critically illness].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2016 May;28(5):396-400. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2016. PMID: 29920026 Chinese.
-
[Evaluation of coagulation disorders with thrombelastography in patients with sepsis].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2016 Feb;28(2):153-8. doi: 10.3760/cma.j.issn.2095-4352.2016.02.013. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2016. PMID: 26911948 Chinese.
-
AGA Clinical Practice Update: Coagulation in Cirrhosis.Gastroenterology. 2019 Jul;157(1):34-43.e1. doi: 10.1053/j.gastro.2019.03.070. Epub 2019 Apr 12. Gastroenterology. 2019. PMID: 30986390 Review.
-
Review article: the prothrombin time test as a measure of bleeding risk and prognosis in liver disease.Aliment Pharmacol Ther. 2007 Jul 15;26(2):141-8. doi: 10.1111/j.1365-2036.2007.03369.x. Aliment Pharmacol Ther. 2007. PMID: 17593061 Review.
Cited by
-
Tracheostomy in critically ill liver disease patients with coagulopathy: A retrospective study at a tertiary center.Int J Crit Illn Inj Sci. 2020 Oct-Dec;10(4):195-199. doi: 10.4103/IJCIIS.IJCIIS_106_19. Epub 2020 Dec 29. Int J Crit Illn Inj Sci. 2020. PMID: 33850828 Free PMC article.
-
Bleeding assessment and bleeding severity in thrombocytopenic patients undergoing invasive procedures.Transfusion. 2020 Mar;60(3):637-649. doi: 10.1111/trf.15670. Epub 2020 Jan 31. Transfusion. 2020. PMID: 32003910 Free PMC article. Review. No abstract available.
-
Comparison of Thromboelastography and Conventional Coagulation Tests in Patients With Severe Liver Disease.Clin Appl Thromb Hemost. 2020 Jan-Dec;26:1076029620925915. doi: 10.1177/1076029620925915. Clin Appl Thromb Hemost. 2020. PMID: 32496878 Free PMC article.
-
Efficacy of using thromboelastography to detect coagulation function and platelet function in patients with acute cerebral infarction.Acta Neurol Belg. 2021 Dec;121(6):1661-1667. doi: 10.1007/s13760-020-01456-6. Epub 2020 Aug 5. Acta Neurol Belg. 2021. PMID: 32757100
-
Prediction and prevention of post-procedural bleedings in patients with cirrhosis.Clin Mol Hepatol. 2025 Feb;31(Suppl):S205-S227. doi: 10.3350/cmh.2024.0928. Epub 2025 Feb 18. Clin Mol Hepatol. 2025. PMID: 39962975 Free PMC article. Review.
References
-
- Lisman T, Porte RJ. Rebalanced hemostasis in patients with liver disease: Evidence and clinical consequences. Blood. 2010;116:878–85. - PubMed
-
- Tripodi A, Salerno F, Chantarangkul V, Clerici M, Cazzaniga M, Primignani M, et al. Evidence of normal thrombin generation in cirrhosis despite abnormal conventional coagulation tests. Hepatology. 2005;41:553–8. - PubMed
-
- Segal JB, Dzik WH. Transfusion Medicine/Hemostasis Clinical Trials Network. Paucity of studies to support that abnormal coagulation test results predict bleeding in the setting of invasive procedures: An evidence-based review. Transfusion. 2005;45:1413–25. - PubMed
-
- Dupont J, Messiant F, Declerck N, Tavernier B, Jude B, Durinck L, et al. Liver transplantation without the use of fresh frozen plasma. Anesth Analg. 1996;83:681–6. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical