

Attenuation of postoperative adhesions using a modeled manual therapy
- PMID: 28574997
- PMCID: PMC5456066
- DOI: 10.1371/journal.pone.0178407
Attenuation of postoperative adhesions using a modeled manual therapy
Abstract
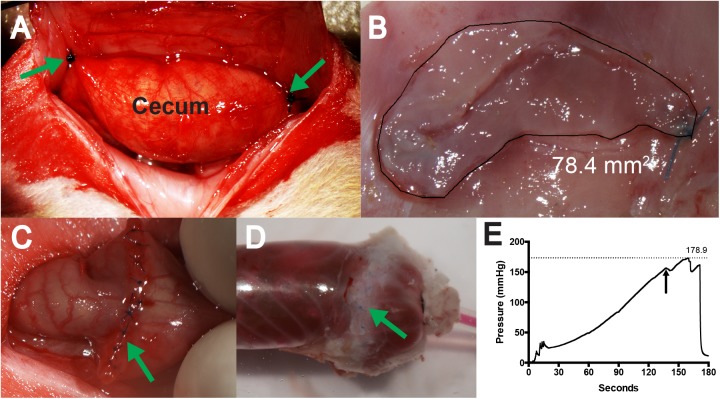
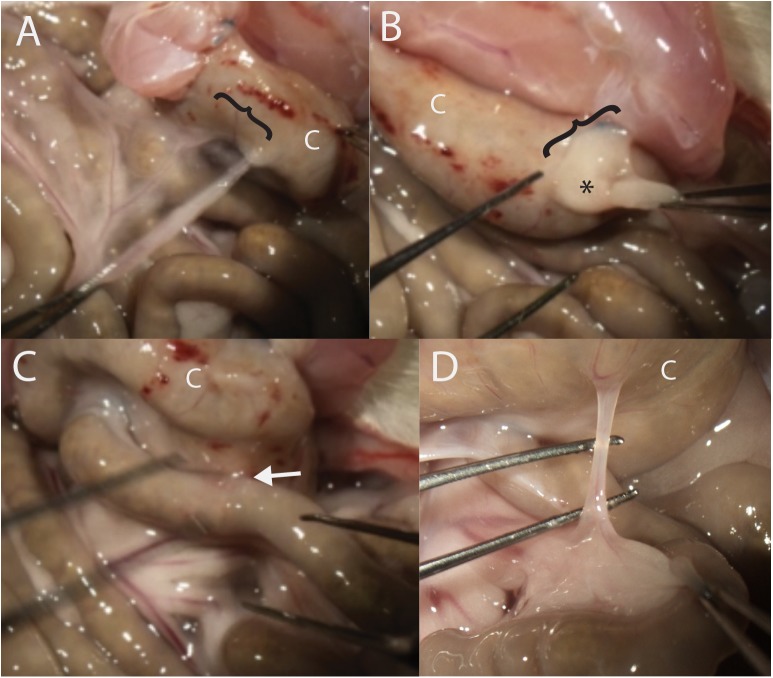
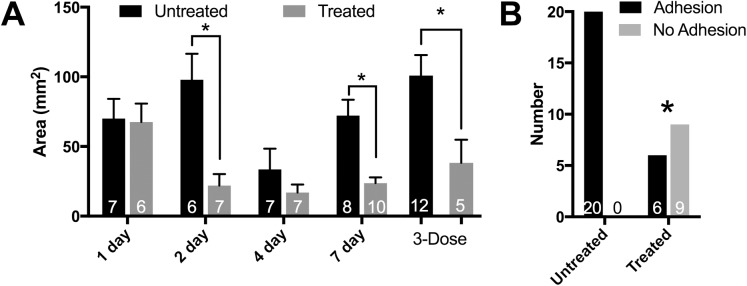
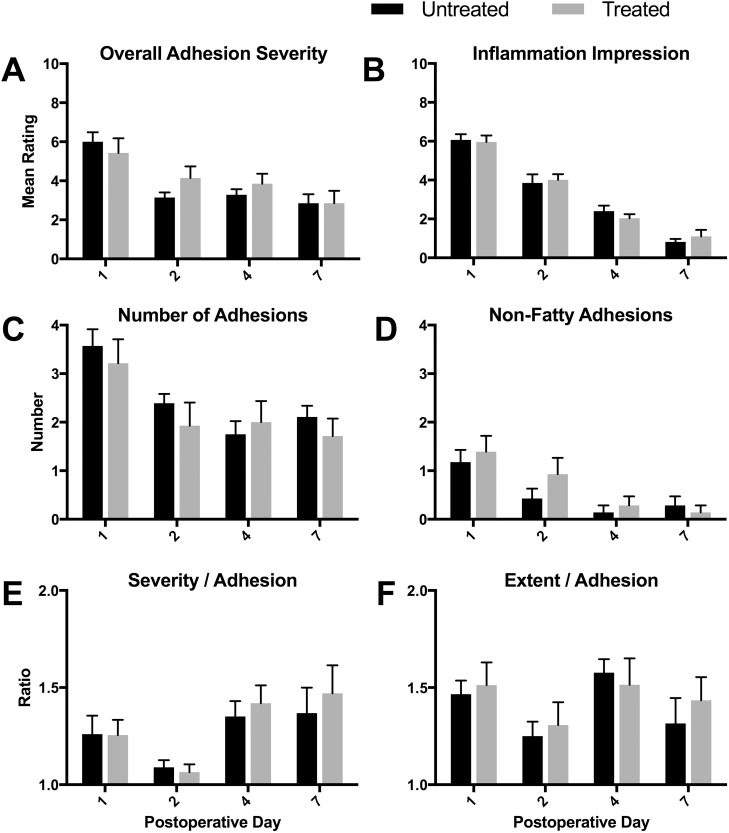
Postoperative adhesions are pathological attachments that develop between abdominopelvic structures following surgery. Considered unavoidable and ubiquitous, postoperative adhesions lead to bowel obstructions, infertility, pain, and reoperations. As such, they represent a substantial health care challenge. Despite over a century of research, no preventive treatment exists. We hypothesized that postoperative adhesions develop from a lack of movement of the abdominopelvic organs in the immediate postoperative period while rendered immobile by surgery and opiates, and tested whether manual therapy would prevent their development. In a modified rat cecal abrasion model, rats were allocated to receive treatment with manual therapy or not, and their resulting adhesions were quantified. We also characterized macrophage phenotype. In separate experiments we tested the safety of the treatment on a strictureplasty model, and also the efficacy of the treatment following adhesiolysis. We show that the treatment led to reduced frequency and size of cohesive adhesions, but not other types of adhesions, such as those involving intraperitoneal fatty structures. This effect was associated with a delay in the appearance of trophic macrophages. The treatment did not inhibit healing or induce undesirable complications following strictureplasty. Our results support that that maintained movements of damaged structures in the immediate postoperative period has potential to act as an effective preventive for attenuating cohesive postoperative adhesion development. Our findings lay the groundwork for further research, including mechanical and pharmacologic approaches to maintain movements during healing.
Conflict of interest statement
Figures
Similar articles
-
A pectin-honey hydrogel prevents postoperative intraperitoneal adhesions in a rat model.BMC Vet Res. 2017 Feb 17;13(1):55. doi: 10.1186/s12917-017-0965-z. BMC Vet Res. 2017. PMID: 28212637 Free PMC article.
-
A hyaluronate based gel for the prevention of postsurgical adhesions: evaluation in two animal species.Fertil Steril. 1996 Nov;66(5):814-21. Fertil Steril. 1996. PMID: 8893691
-
Visceral mobilization can lyse and prevent peritoneal adhesions in a rat model.J Bodyw Mov Ther. 2012 Jan;16(1):76-82. doi: 10.1016/j.jbmt.2011.02.004. Epub 2011 Apr 9. J Bodyw Mov Ther. 2012. PMID: 22196431
-
Adhesions: preventive strategies.Eur J Surg Suppl. 1997;(577):32-9. Eur J Surg Suppl. 1997. PMID: 9076450 Review.
-
Adhesions: pathogenesis and prevention-panel discussion and summary.Eur J Surg Suppl. 1997;(577):56-62. Eur J Surg Suppl. 1997. PMID: 9076453 Review.
Cited by
-
Physiological Responses Induced by Manual Therapy in Animal Models: A Scoping Review.Front Neurosci. 2020 May 8;14:430. doi: 10.3389/fnins.2020.00430. eCollection 2020. Front Neurosci. 2020. PMID: 32457570 Free PMC article.
-
Evaluating massage therapy for radiation-induced fibrosis in rats: preliminary findings and palpation results.Cancer Biol Ther. 2024 Dec 31;25(1):2436694. doi: 10.1080/15384047.2024.2436694. Epub 2024 Dec 2. Cancer Biol Ther. 2024. PMID: 39620471 Free PMC article.
-
The Influence of a Single Instrument-Assisted Manual Therapy (IAMT) for the Lower Back on the Structural and Functional Properties of the Dorsal Myofascial Chain in Female Soccer Players: A Randomised, Placebo-Controlled Trial.J Clin Med. 2022 Nov 30;11(23):7110. doi: 10.3390/jcm11237110. J Clin Med. 2022. PMID: 36498690 Free PMC article.
-
Irritable Bowel Syndrome-Like Symptoms in Quiescent Inflammatory Bowel Disease: A Practical Approach to Diagnosis and Treatment of Organic Causes.Dig Dis Sci. 2023 Nov;68(11):4081-4097. doi: 10.1007/s10620-023-08095-w. Epub 2023 Sep 11. Dig Dis Sci. 2023. PMID: 37695549 Free PMC article. Review.
-
Functional and Structural Long-Term Effects of Repetitive Instrument-Assisted Manual Therapy (IAMT) of the Lumbar Back on the Dorsal Myofascial Chain Among Female Soccer Players: A Randomized, Placebo-Controlled Pilot Trial.Cureus. 2024 Sep 13;16(9):e69337. doi: 10.7759/cureus.69337. eCollection 2024 Sep. Cureus. 2024. PMID: 39398775 Free PMC article.
References
-
- Stanciu D, Menzies D. The magnitude of adhesion-related problems. Colorectal Dis. 2007;9:35–8. doi: 10.1111/j.1463-1318.2007.01346.x - DOI - PubMed
-
- Parker MC, Wilson MS, van GH, Moran BJ, Jeekel J, Duron JJ, et al. Adhesions and colorectal surgery—call for action. Colorectal Dis. 2007;9:66–72. doi: 10.1111/j.1463-1318.2007.01342.x - DOI - PubMed
-
- Beck DE, Opelka FG, Bailey HR, Rauh SM, Pashos CL. Incidence of small-bowel obstruction and adhesiolysis after open colorectal and general surgery. Diseases of the Colon & Rectum. 1999;42(2):241–8. - PubMed
-
- Kresch AJ, Seifer DB, Sachs LB, Barrese I. Laparoscopy in 100 women with chronic pelvic pain. Obstet Gynecol. 1984;64(5):672–4. Epub 1984/11/01. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
