

CA-125 in Disease Progression and Treatment of Lymphangioleiomyomatosis
- PMID: 28576630
- PMCID: PMC6026218
- DOI: 10.1016/j.chest.2017.05.018
CA-125 in Disease Progression and Treatment of Lymphangioleiomyomatosis
Abstract
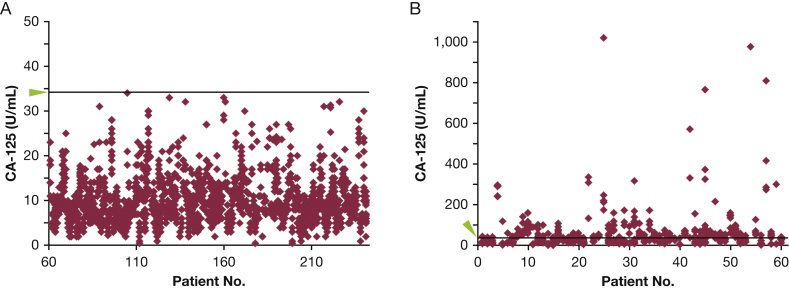
Background: Lymphangioleiomyomatosis (LAM) is a destructive lung disease of women caused by proliferation of neoplastic-like LAM cells, with mutations in the TSC1/2 tumor suppressor genes. Based on case reports, levels of cancer antigen 125 (CA-125), an ovarian cancer biomarker, can be elevated in patients with LAM. We hypothesized that elevated serum CA-125 levels seen in some patients with LAM were due to LAM, not other malignancies, and might respond to sirolimus treatment.
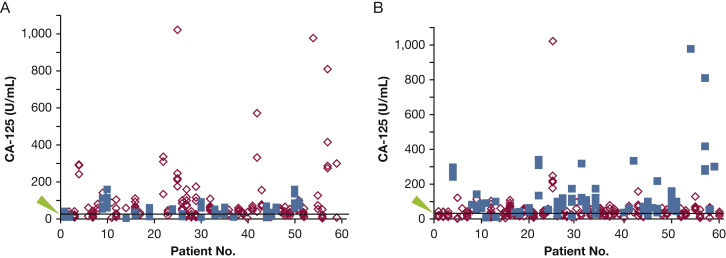
Methods: Serum CA-125 levels were measured for 241 patients at each visit. Medical records were reviewed for co-morbidities, disease progression, and response to sirolimus treatment. CA-125 expression in LAM cells was determined by using immunohistochemical analysis.
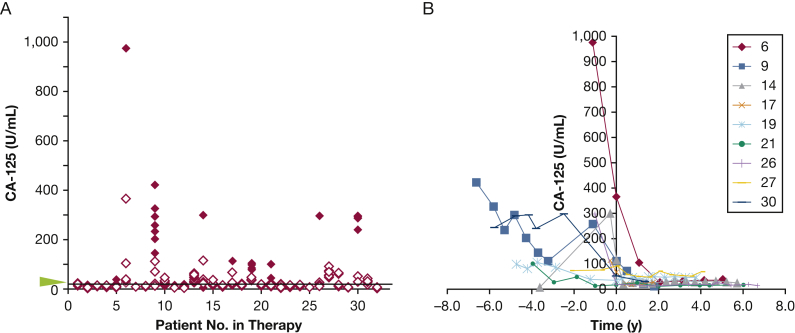
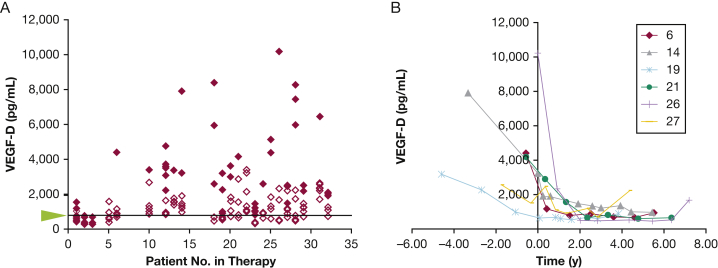
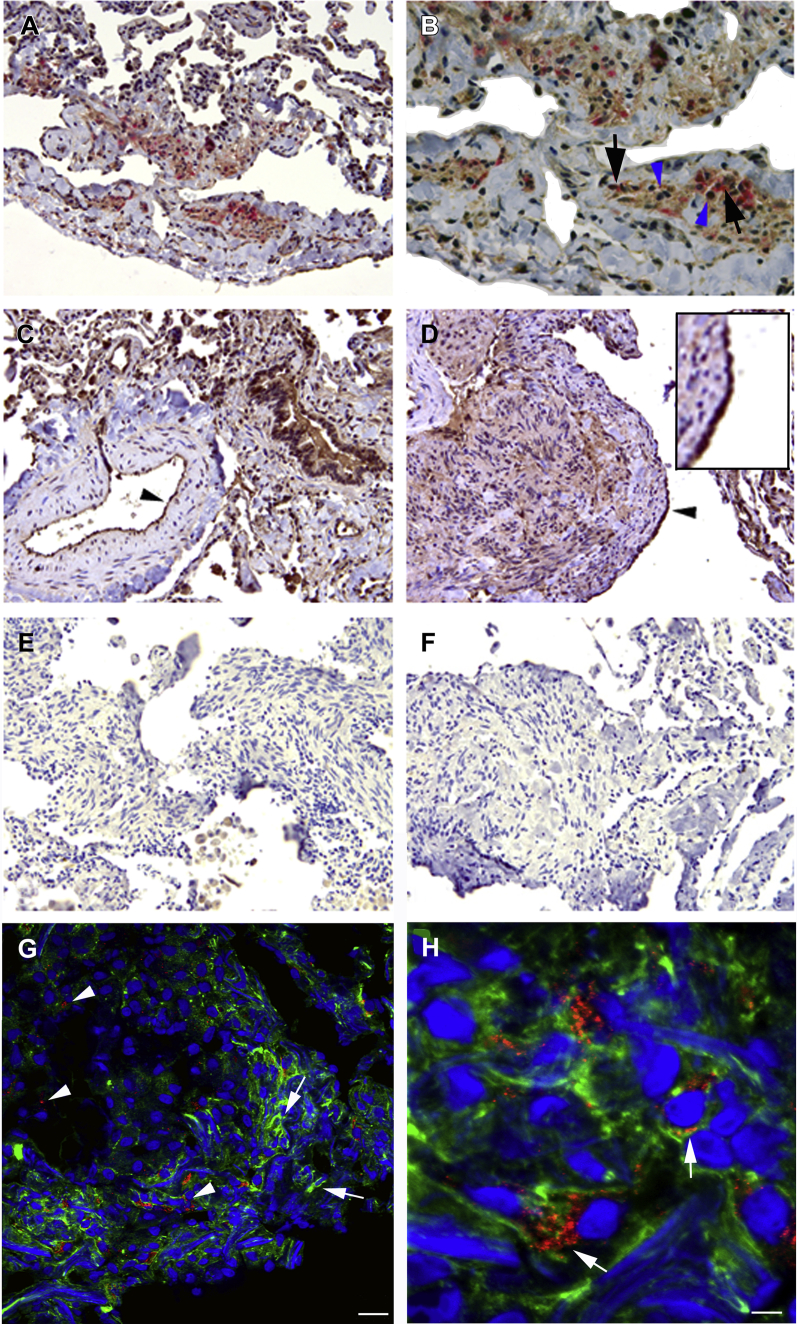
Results: Almost 25% of patients with LAM had at least one elevated serum CA-125 measurement. Higher serum CA-125 levels correlated with lower FEV1, premenopausal status, and pleural effusion in a multivariate model (each P < .001). Serum CA-125 levels decreased following sirolimus treatment (P = .002). CA-125 and α-smooth muscle actin were co-expressed in LAM lung nodules.
Conclusions: Higher serum CA-125 levels were associated with pleural effusions and reduced pulmonary function and were decreased with sirolimus therapy. LAM cells express CA-125. Some elevated serum CA-125 levels may reflect serosal membrane involvement.
Keywords: CA-125; lymphangioleiomyomatosis; mTOR; pleural effusion; tuberous sclerosis.
Copyright © 2017. Published by Elsevier Inc.
Figures
Comment in
-
The 10,000-Piece Puzzle of Lymphangioleiomyomatosis.Chest. 2018 Feb;153(2):298-299. doi: 10.1016/j.chest.2017.07.027. Chest. 2018. PMID: 29406212 No abstract available.
References
-
- Benjamin D., Colombi M., Moroni C., Hall M.N. Rapamycin passes the torch: a new generation of mTOR inhibitors. Nat Rev Drug Discov. 2011;10(11):868–880. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
