

CMV and BKPyV Infections in Renal Transplant Recipients Receiving an mTOR Inhibitor-Based Regimen Versus a CNI-Based Regimen: A Systematic Review and Meta-Analysis of Randomized, Controlled Trials
- PMID: 28576905
- PMCID: PMC5544521
- DOI: 10.2215/CJN.13221216
CMV and BKPyV Infections in Renal Transplant Recipients Receiving an mTOR Inhibitor-Based Regimen Versus a CNI-Based Regimen: A Systematic Review and Meta-Analysis of Randomized, Controlled Trials
Abstract
Background and objectives: The objective of this meta-analysis is to compare the incidences of cytomegalovirus and BK polyoma virus infections in renal transplant recipients receiving a mammalian target of rapamycin inhibitor (mTOR)-based regimen compared with a calcineurin inhibitor-based regimen.
Design, setting, participants, & measurements: We conducted a comprehensive search for randomized, controlled trials up to January of 2016 addressing our objective. Other outcomes included acute rejection, graft loss, serious adverse events, proteinuria, wound-healing complications, and eGFR. Two review authors selected eligible studies, abstracted data, and assessed risk of bias. We assessed quality of evidence using the Grading of Recommendations Assessment, Development and Evaluation methodology.
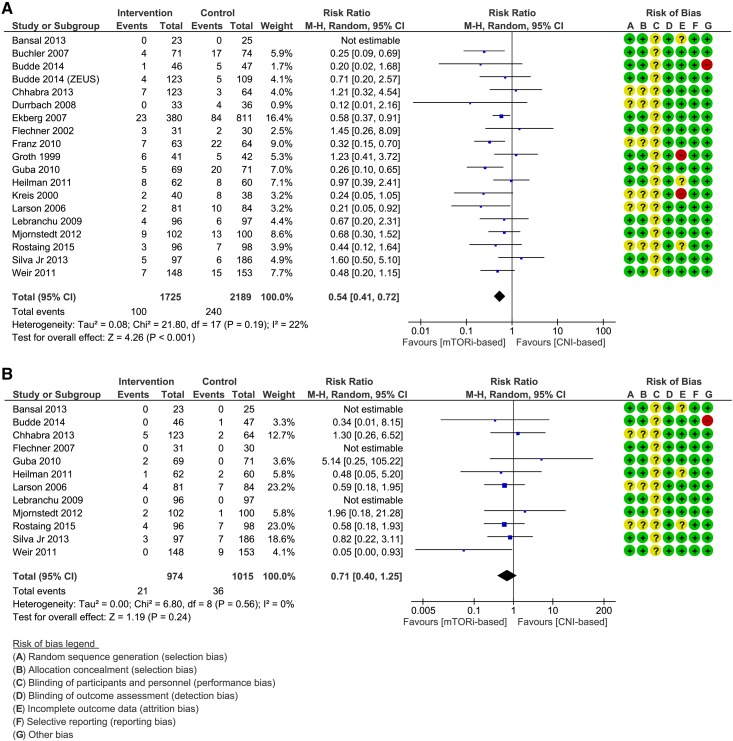
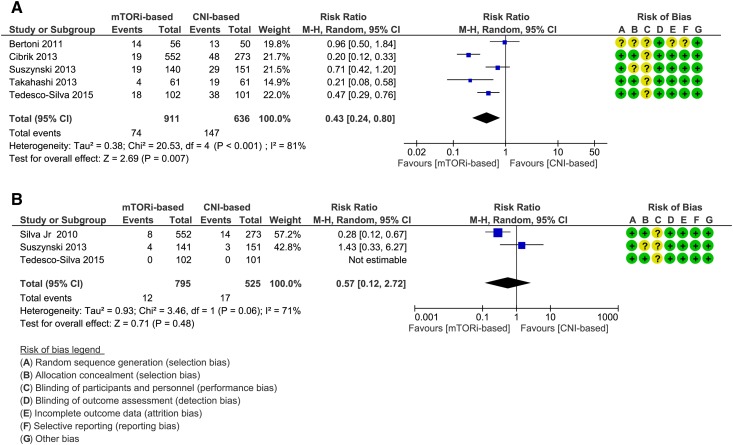
Results: We included 28 randomized, controlled trials with 6211 participants classified into comparison 1: mTOR inhibitor versus calcineurin inhibitor and comparison 2: mTOR inhibitor plus reduced dose of calcineurin inhibitor versus regular dose of calcineurin inhibitor. Results showed decreased incidence of cytomegalovirus infection in mTOR inhibitor-based group in both comparison 1 (risk ratio, 0.54; 95% confidence interval, 0.41 to 0.72), with high quality of evidence, and comparison 2 (risk ratio, 0.43; 95% confidence interval, 0.24 to 0.80), with moderate quality of evidence. The available evidence neither confirmed nor ruled out a reduction of BK polyoma virus infection in mTOR inhibitor-based group in both comparisons. Secondary outcomes revealed more serious adverse events and acute rejections in mTOR inhibitor-based group in comparison 1 and no difference in comparison 2. There was no difference in graft loss in both comparisons. eGFR was higher in the mTOR inhibitor-based group in comparison 1 (mean difference =4.07 ml/min per 1.73 m2; 95% confidence interval, 1.34 to 6.80) and similar to the calcineurin inhibitor-based group in comparison 2. More proteinuria and wound-healing complications occurred in the mTOR inhibitor-based groups.
Conclusions: We found moderate- to high-quality evidence of reduced risk of cytomegalovirus infection in renal transplant recipients in the mTOR inhibitor-based compared with the calcineurin inhibitor-based regimen. Our review also suggested that a combination of a mTOR inhibitor and a reduced dose of calcineurin inhibitor may be associated with similar eGFR and rates of acute rejections and serious adverse events compared with a standard calcineurin inhibitor-based regimen at the expense of higher incidence of proteinuria and wound-healing complications.
Keywords: Assessment; BK virus; Calcineurin; Calcineurin Inhibitors; Calcineurin inhibitor; Confidence Intervals; Cytomegalovirus Infections; Incidence; Meta-analysis; Odds Ratio; Polyomavirus; Randomized Controlled Trials as Topic; Risk; Sirolimus; Wound Healing; cyclosporine; cytomegalovirus; everolimus; glomerular filtration rate; immunosuppression; kidney transplantation; proteinuria; sirolimus; tacrolimus.
Copyright © 2017 by the American Society of Nephrology.
Figures

References
-
- De Keyzer K, Van Laecke S, Peeters P, Vanholder R: Human cytomegalovirus and kidney transplantation: A clinician’s update. Am J Kidney Dis 58: 118–126, 2011 - PubMed
-
- Hirsch HH, Brennan DC, Drachenberg CB, Ginevri F, Gordon J, Limaye AP, Mihatsch MJ, Nickeleit V, Ramos E, Randhawa P, Shapiro R, Steiger J, Suthanthiran M, Trofe J: Polyomavirus-associated nephropathy in renal transplantation: Interdisciplinary analyses and recommendations. Transplantation 79: 1277–1286, 2005 - PubMed
-
- Wiseman AC: Polyomavirus nephropathy: A current perspective and clinical considerations. Am J Kidney Dis 54: 131–142, 2009 - PubMed
-
- Kidney Disease: Improving Global Outcomes (KDIGO) Transplant Work Group : KDIGO clinical practice guideline for the care of kidney transplant recipients. Am J Transplant 9[Suppl 3]: S1–S155, 2009 - PubMed
-
- Nashan B, Gaston R, Emery V, Säemann MD, Mueller NJ, Couzi L, Dantal J, Shihab F, Mulgaonkar S, Seun Kim Y, Brennan DC: Review of cytomegalovirus infection findings with mammalian target of rapamycin inhibitor-based immunosuppressive therapy in de novo renal transplant recipients. Transplantation 93: 1075–1085, 2012 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
