

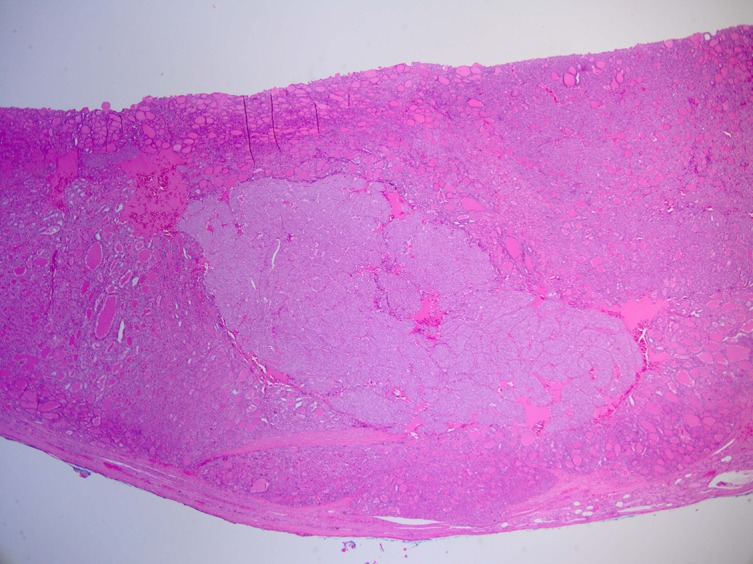
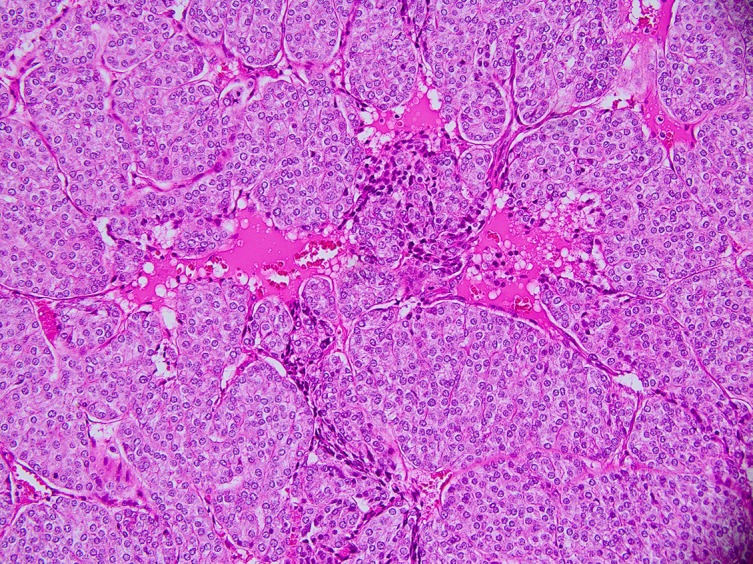
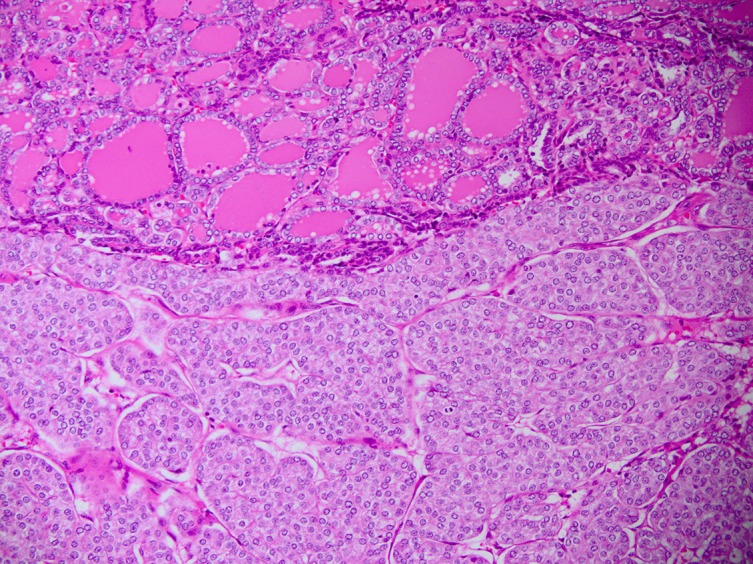
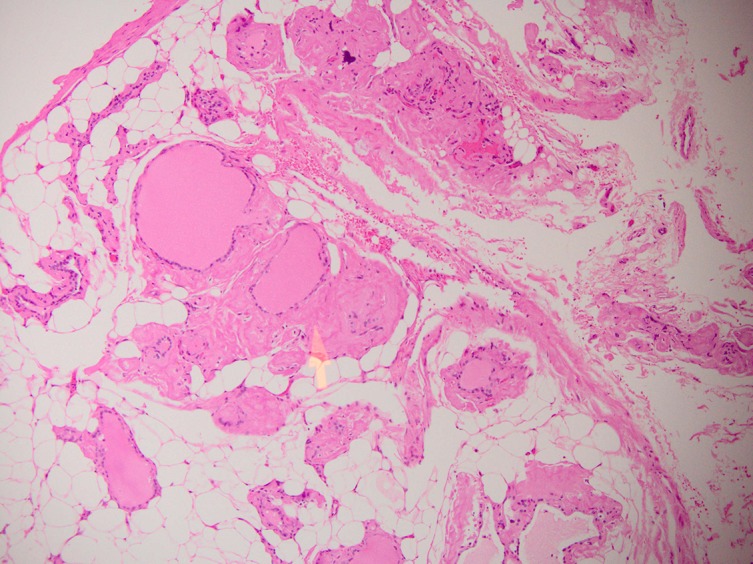
Insular carcinoma arising on a background of follicular carcinoma, thyrolipomatosis and amyloid goitre
- PMID: 28576912
- PMCID: PMC5534650
- DOI: 10.1136/bcr-2017-219747
Insular carcinoma arising on a background of follicular carcinoma, thyrolipomatosis and amyloid goitre
Abstract
A 67-year-old man was referred with a history of a right-sided neck lump and dysphonia, secondary to a lesion in the thyroid gland. After undergoing a total thyroidectomy, he was found to have an exceedingly rare combination of follicular carcinoma, insular carcinoma, thyrolipomatosis and an amyloid goitre in his thyroid gland. He subsequently underwent further radioactive iodine ablation and has been in remission. He was also later incidentally diagnosed with systemic amyloidosis, which explained the amyloid deposition in his thyroid gland.
Keywords: Endocrine cancer; Head and neck cancer; Head and neck surgery; Pathology; Thyroid disease.
© BMJ Publishing Group Ltd (unless otherwise stated in the text of the article) 2017. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
Figures

References
-
- Dhayagude RG. Massive fatty infiltration in a colloid goiter. Arch Pathol 1942;33:357–60.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical