

Prevention of acute kidney injury and protection of renal function in the intensive care unit: update 2017 : Expert opinion of the Working Group on Prevention, AKI section, European Society of Intensive Care Medicine
- PMID: 28577069
- PMCID: PMC5487598
- DOI: 10.1007/s00134-017-4832-y
Prevention of acute kidney injury and protection of renal function in the intensive care unit: update 2017 : Expert opinion of the Working Group on Prevention, AKI section, European Society of Intensive Care Medicine
Abstract
Background: Acute kidney injury (AKI) in the intensive care unit is associated with significant mortality and morbidity.
Objectives: To determine and update previous recommendations for the prevention of AKI, specifically the role of fluids, diuretics, inotropes, vasopressors/vasodilators, hormonal and nutritional interventions, sedatives, statins, remote ischaemic preconditioning and care bundles.
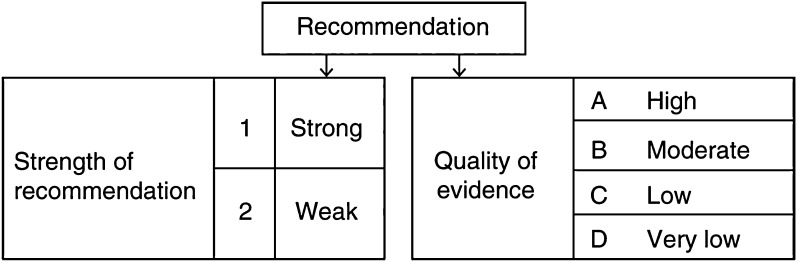
Method: A systematic search of the literature was performed for studies published between 1966 and March 2017 using these potential protective strategies in adult patients at risk of AKI. The following clinical conditions were considered: major surgery, critical illness, sepsis, shock, exposure to potentially nephrotoxic drugs and radiocontrast. Clinical endpoints included incidence or grade of AKI, the need for renal replacement therapy and mortality. Studies were graded according to the international GRADE system.
Results: We formulated 12 recommendations, 13 suggestions and seven best practice statements. The few strong recommendations with high-level evidence are mostly against the intervention in question (starches, low-dose dopamine, statins in cardiac surgery). Strong recommendations with lower-level evidence include controlled fluid resuscitation with crystalloids, avoiding fluid overload, titration of norepinephrine to a target MAP of 65-70 mmHg (unless chronic hypertension) and not using diuretics or levosimendan for kidney protection solely.
Conclusion: The results of recent randomised controlled trials have allowed the formulation of new recommendations and/or increase the strength of previous recommendations. On the other hand, in many domains the available evidence remains insufficient, resulting from the limited quality of the clinical trials and the poor reporting of kidney outcomes.
Keywords: Acute kidney injury; Prevention; Recommendations; Systematic review; Vasopressors; Volume expansion.
Conflict of interest statement
MJ has received honoraria or research support from Baxter Healthcare Corp, AM-Pharma, CLS Behring, Fresenius and Astute Medical. WD declares no conflicts of interest. LF has received honoraria and research support from Astute Medical, Fresenius, Baxter Gambro Renal and Orthoclinical Diagnostics. PH had received research grants from Baxter, AM Pharma, Bellco, and Pfizer EH received speaker’s fees from Alexion and Astute Medical, and a research grant from Bellco. MO has received honoraria and research funding from Fresenius Medical Care and Baxter Gambro. HO has financial congress support from Dirinco (Netherlands) and speaker’s honoraria from Fresenius and Gambro/Baxter. MS declares no conflicts of interest.
Figures
References
-
- Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group KDIGO clinical practice guideline for acute kidney injury. Kidney Int Suppl. 2012;2:1–138. doi: 10.1038/kisup.2012.1. - DOI
-
- Kirwan CJ, Blunden MJ, Dobbie H, James A, Nedungadi A, Prowle JR. Critically ill patients requiring acute renal replacement therapy are at an increased risk of long-term renal dysfunction, but rarely receive specialist nephrology follow-up. Nephron. 2015;129:164–170. doi: 10.1159/000371448. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
