

Aeroembolism in left atrium during catheter ablation of atrial fibrillation in a patient with dextrocardia: a case report and review of the literature
- PMID: 28577360
- PMCID: PMC5457732
- DOI: 10.1186/s12872-017-0581-7
Aeroembolism in left atrium during catheter ablation of atrial fibrillation in a patient with dextrocardia: a case report and review of the literature
Abstract
Background: Air embolus penetrating into heart chamber as a complication during percutaneous radiofrequency catheter ablation has been infrequently reported.
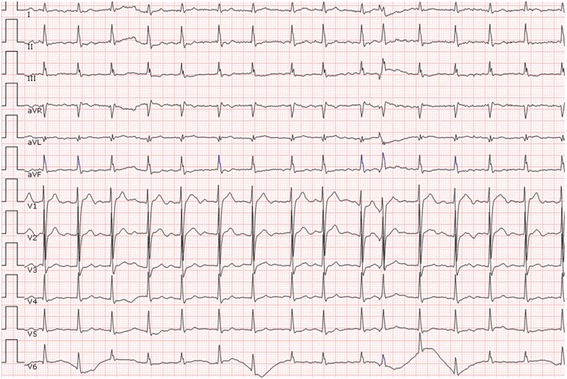
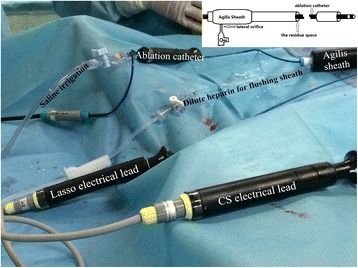
Case presentation: A 55-year-old man with dextrocardia who suffered from abdominal pain was suspected to have multiple arterial thromboembolisms, which might have originated from left atrium thrombosis since he had atrial fibrillation. He received oral anticoagulant therapy and catheter ablation of the arrhythmia. During the ablation procedure, an iatrogenic aeroembolism penetrated into the left atrium due to improper operation. Ultimately, the entire air embolus was extracted from the patient, who was free of any aeroembolism events thereafter.
Conclusions: It is essential for an operator to pay full attention to all details of the procedure to avoid an aeroembolism during catheter ablation. In case of aeroembolism, removal by aspiration is an optimal and effective treatment.
Keywords: Aeroembolism; Atrial fibrillation; Case report; Catheter ablation; Dextrocardia.
Figures


References
-
- Camm AJ, Lip GY, De Caterina R, Savelieva I, Atar D, Hohnloser SH, et al. ESC Committee for practice guidelines (CPG). 2012 focused update of the ESC guidelines for the management of atrial fibrillation: an update of the 2010 ESCGuidelines for the management of atrial fibrillation. Developed with the special contribution of the European heart rhythm association. Eur Heart J. 2012;33:2719–47. - PubMed
-
- Cappato R, Calkins H, Chen SA, Davies W, Iesaka Y, Kalman J, et al. Worldwide survey on the methods, efficacy, and safety of catheter ablation for human atrial fibrillation. Circulation. 2005;111:1100–5. - PubMed
-
- Herweg B, Sichrovsky T, Polosajian L, Vloka M, Rozenshtein A, Steinberg JS. Anatomic substrate, procedural results, and clinical outcome of ultrasound-guided left atrial-pulmonary vein disconnection for treatment of atrial fibrillation. Am J Cardiol. 2005;95:871–875. doi: 10.1016/j.amjcard.2004.12.019. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
