

Patterns of relapse in primary central nervous system lymphoma: inferences regarding the role of the neuro-vascular unit and monoclonal antibodies in treating occult CNS disease
- PMID: 28577579
- PMCID: PMC5457655
- DOI: 10.1186/s12987-017-0064-3
Patterns of relapse in primary central nervous system lymphoma: inferences regarding the role of the neuro-vascular unit and monoclonal antibodies in treating occult CNS disease
Abstract
Background and purpose: The radiologic features and patterns of primary central nervous system lymphoma (PCNSL) at initial presentation are well described. High response rates can be achieved with first-line high-dose methotrexate (HD-MTX) based regimens, yet many relapse within 2 years of diagnosis. We describe the pattern of relapse and review the potential mechanisms involved in relapse.
Methods: We identified 78 consecutive patients who attained complete radiographic response (CR) during or after first-line treatment for newly diagnosed PCNSL (CD20+, diffuse large B cell type). Patients were treated with HD-MTX based regimen in conjunction with blood-brain barrier disruption (HD-MTX/BBBD); 44 subsequently relapsed. Images and medical records of these 44 consecutive patients were retrospectively reviewed. The anatomical location of enhancing lesions at initial diagnosis and at the time of relapse were identified and compared.
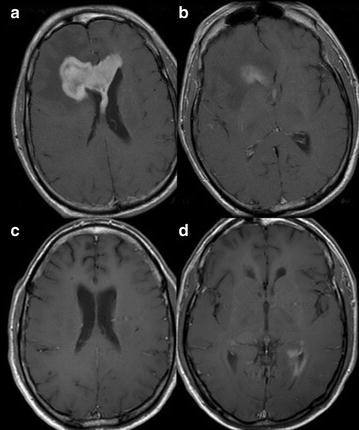
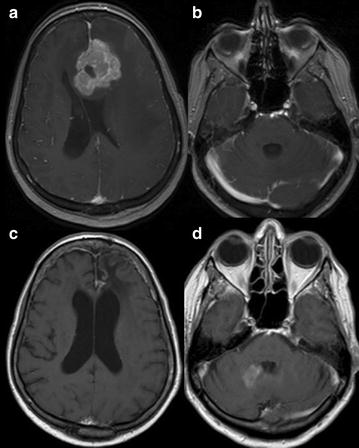
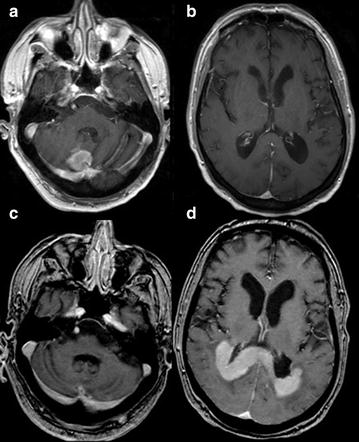
Results: 37/44 patients fulfilled inclusion criteria and had new measureable enhancing lesions at relapse; the pattern and location of relapse of these 37 patients were identified. At relapse, the new enhancement was at a spatially distinct site in 30 of 37 patients. Local relapse was found only in seven patients.
Discussion: Unlike gliomas, the majority of PCNSL had radiographic relapse at spatially distinct anatomical locations within the brain behind a previously intact neurovascular unit (NVU), and in few cases outside, the central nervous system (CNS). This may suggest either (1) reactivation of occult reservoirs behind an intact NVU in the CNS (or ocular) or (2) seeding from bone marrow or other extra CNS sites.
Conclusion: Recognizing patterns of relapse is key for early detection and may provide insight into potential mechanisms of relapse as well as help develop strategies to extend duration of complete response.
Figures

References
-
- Hoang-Xuan K, Bessell E, Bromberg J, Hottinger AF, Preusser M, Ruda R, Schlegel U, Siegal T, Soussain C, Abacioglu U, et al. Diagnosis and treatment of primary CNS lymphoma in immunocompetent patients: guidelines from the European Association for Neuro-Oncology. Lancet Oncol. 2015;16:e322–e332. doi: 10.1016/S1470-2045(15)00076-5. - DOI - PubMed
-
- Abrey LE, Batchelor TT, Ferreri AJ, Gospodarowicz M, Pulczynski EJ, Zucca E, Smith JR, Korfel A, Soussain C, DeAngelis LM, et al. Report of an international workshop to standardize baseline evaluation and response criteria for primary CNS lymphoma. J Clin Oncol. 2005;23:5034–5043. doi: 10.1200/JCO.2005.13.524. - DOI - PubMed
-
- Thiel E, Korfel A, Martus P, Kanz L, Griesinger F, Rauch M, Roth A, Hertenstein B, von Toll T, Hundsberger T, et al. High-dose methotrexate with or without whole brain radiotherapy for primary CNS lymphoma (G-PCNSL-SG-1): a phase 3, randomised, non-inferiority trial. Lancet Oncol. 2010;11:1036–1047. doi: 10.1016/S1470-2045(10)70229-1. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
