

Alternatives to Traditional Per-Oral Endoscopy for Screening
- PMID: 28577763
- PMCID: PMC6055990
- DOI: 10.1016/j.giec.2017.02.002
Alternatives to Traditional Per-Oral Endoscopy for Screening
Abstract
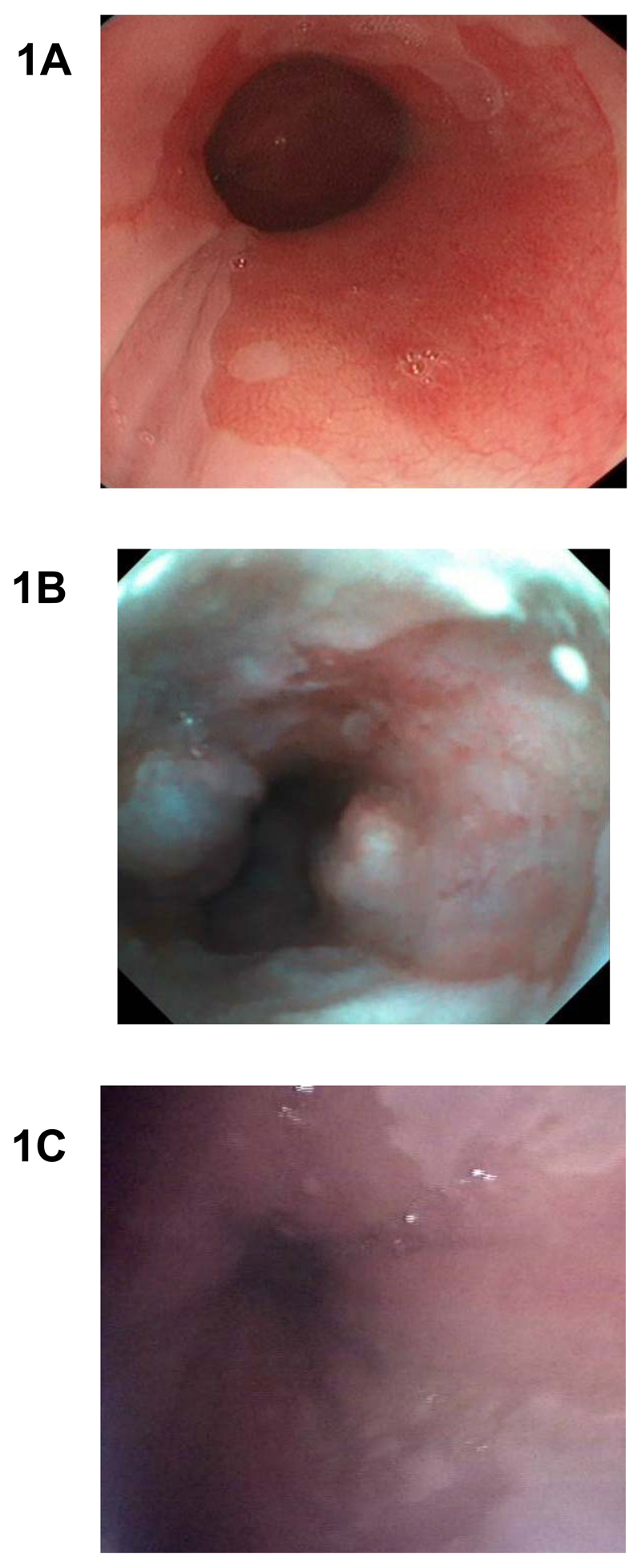
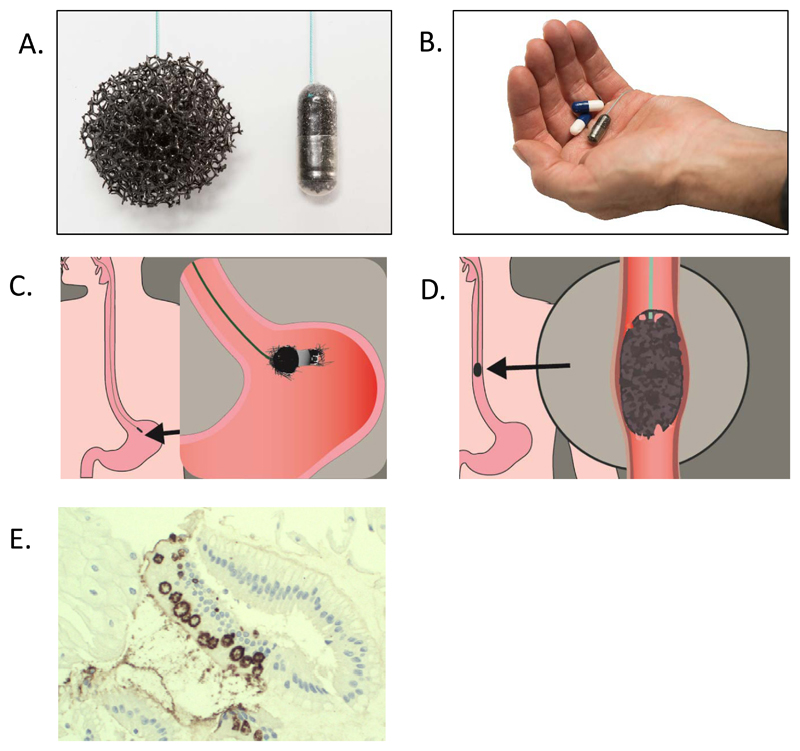
Barrett's esophagus (BE) predisposes patients to esophageal adenocarcinoma. 3 to 6% of individuals with gastro-esophageal reflux disease are estimated to have BE but only 20 to 25% of BE patients are currently diagnosed. The current gold standard for diagnosis of BE is per-oral upper GI endoscopy. As this is not suitable for large-scale screening, a number of alternative methods are currently being investigated: transnasal and video capsule endoscopy, endomicroscopy, cell collection devices like the cytosponge and biomarkers. Some of these are promising, however, well powered studies carried out in relevant screening populations are needed.
Keywords: Barrett’s esophagus; Biomarkers; Cell collection; Endoscopy; Esophageal adenocarcinoma; Screening; Transnasal endoscopy; Video capsule endoscopy.
Copyright © 2017 Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflicts of interest
The authors disclose the following: R.C.F. holds patents on the Cytosponge technology, which has been licensed by MRC Technology to Covidien GI Solutions (now Medtronic). R.C.F. has no direct financial arrangement with Metronic. J.O. has no conflict of interest to declare.
Figures
References
-
- McDonald SA, Lavery D, Wright NA, Jansen M. Barrett oesophagus: lessons on its origins from the lesion itself. Nat Rev Gastroenterol Hepatol. 2015;12(1):50–60. - PubMed
-
- Eloubeidi MA, Mason AC, Desmond RA, El-Serag HB. Temporal trends (1973-1997) in survival of patients with esophageal adenocarcinoma in the United States: a glimmer of hope[quest] The American journal of gastroenterology. 2003;98(7):1627–1633. - PubMed
-
- Cancer Research UK. Oesophageal cancer statistics. [Accessed 25/11/2015];2015 http://www.cancerresearchuk.org/health-professional/cancer-statistics/st....
-
- Edgren G, Adami H-O, Weiderpass E, Nyrén O. A global assessment of the oesophageal adenocarcinoma epidemic. Gut. 2013;62(10):1406–1414. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
