

Psychosine, a marker of Krabbe phenotype and treatment effect
- PMID: 28579020
- PMCID: PMC5548593
- DOI: 10.1016/j.ymgme.2017.05.015
Psychosine, a marker of Krabbe phenotype and treatment effect
Abstract
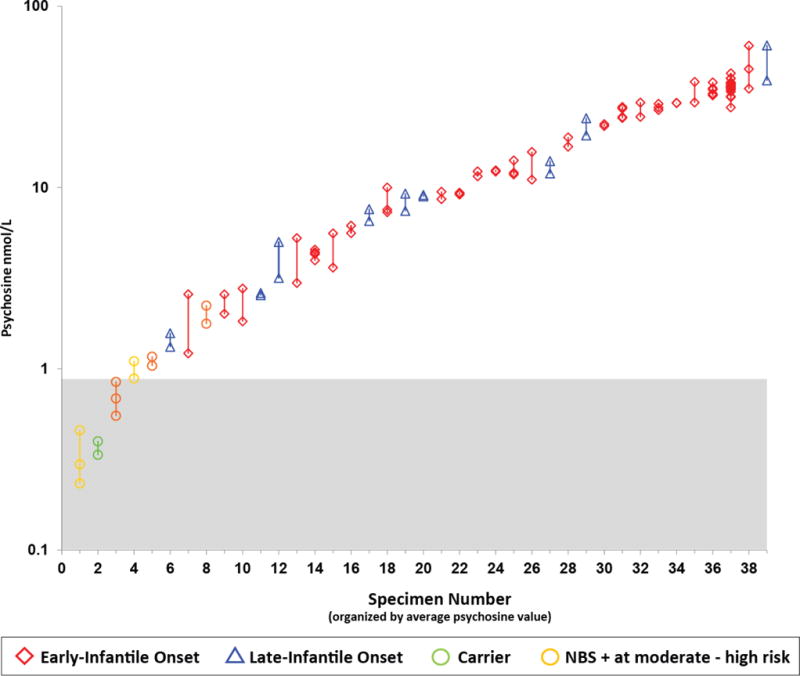
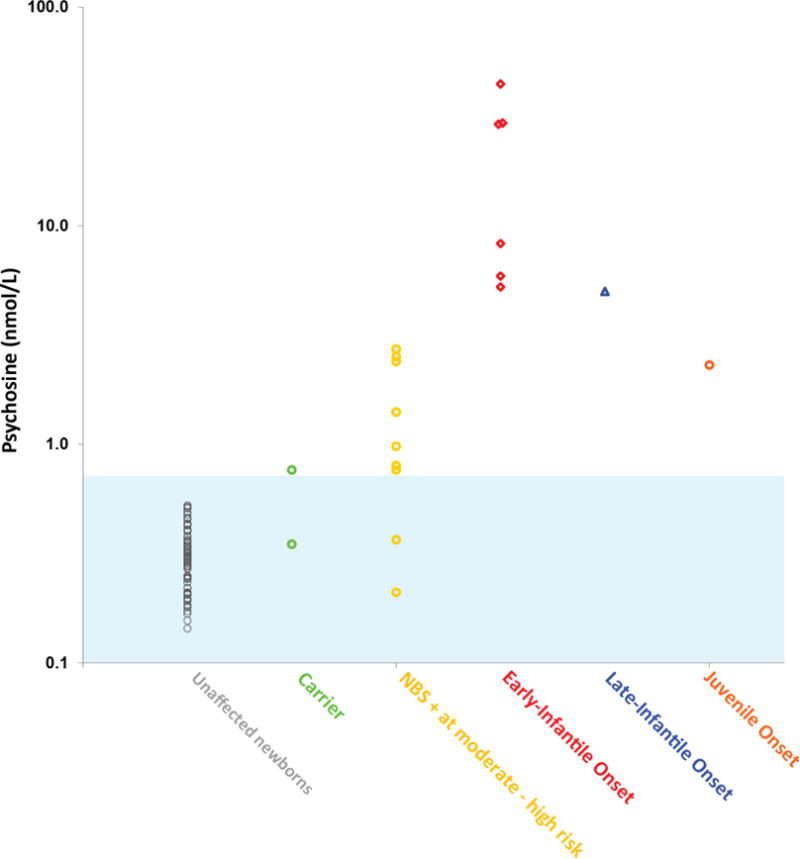
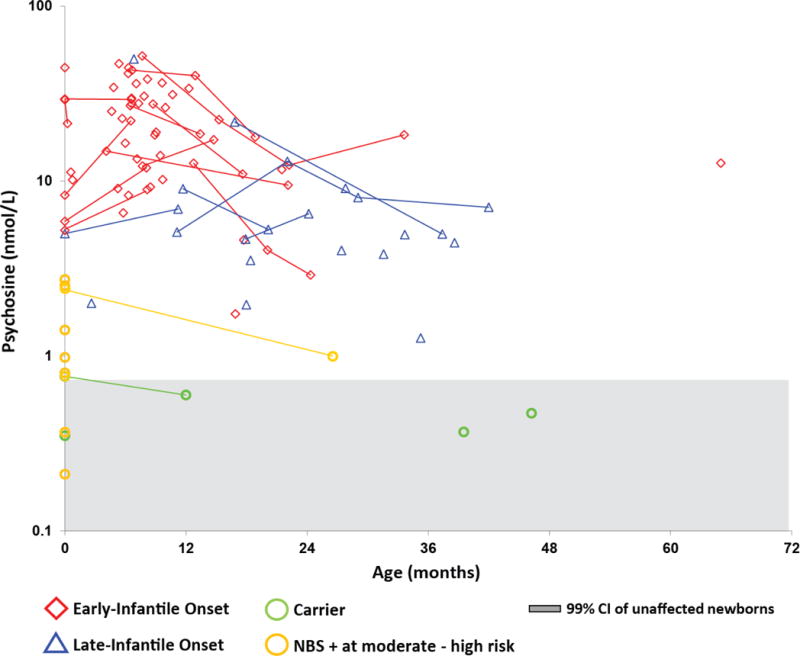
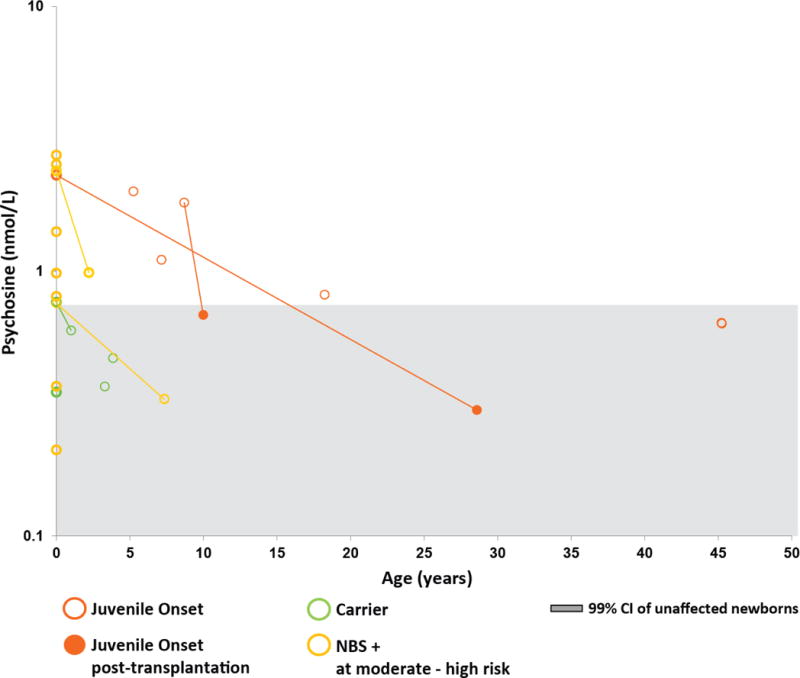
Newborn screening (NBS) for Krabbe disease, a rare neurodegenerative disorder caused by deficient galactocerebrosidase (GALC) enzyme activity, has recently been implemented in a number of US states. However, the spectrum of phenotypic manifestations associated with deficient GALC activity complicates the management of screen-positive newborns and underscores the need to identify clinically relevant biomarkers. Earlier studies with a small number of patients identified psychosine, a substrate of the GALC enzyme, as a potential biomarker for Krabbe disease. In this study, we provide, for the first time, longitudinal data on dried blood spot (DBS) psychosine concentrations in different Krabbe disease phenotypes for both untreated patients and those treated with hematopoietic stem cell transplantation (HSCT). Our cohort included patients previously identified by NBS to be at high risk to develop Krabbe disease. Substantially elevated DBS psychosine concentration during the newborn period was found to be a highly specific marker for infantile Krabbe disease. This finding supports the use of DBS psychosine concentration as a second-tier NBS test to aid in the identification of patients who require urgent evaluation for HSCT. In addition, longitudinal assessments showed that both natural disease progression and treatment with HSCT were associated with decreases in DBS psychosine concentrations. Based on these findings we provide recommendations for the interpretation of psychosine concentrations in DBS specimens collected during the first year of life. Future studies should aim to better delineate the relationship between DBS psychosine concentration and disease onset in patients with later-onset forms of Krabbe disease.
Keywords: Galactosylsphingosine; Globoid cell leukodystrophy; Krabbe disease; Newborn screening; Psychosine; Tandem mass spectrometry.
Copyright © 2017 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Wenger DA. Krabbe Disease. 2000 Jun 19 [Updated 2011 Mar 31] In: Pagon RA, Adam MP, Ardinger HH, et al., editors. GeneReviews® [Internet] Seattle WA: University of Washington, Seattle; 1993–2017. Available from: https://www.ncbi.nlm.nih.gov/books/NBK1238/. Accessed March 6, 2017.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
