

doi: 10.1016/j.healun.2017.05.015.
Epub 2017 May 17.
Potential impact of a shock requirement on adult heart allocation
Affiliations
- PMID: 28579114
- PMCID: PMC6060413
- DOI: 10.1016/j.healun.2017.05.015
Item in Clipboard
Potential impact of a shock requirement on adult heart allocation
J Heart Lung Transplant.
2017 Sep.
No abstract available
Conflict of interest statement
None of the authors has a financial relationship with a commercial entity that has an interest in the subject of the presented manuscript or other conflicts of interest to disclose.
Figures
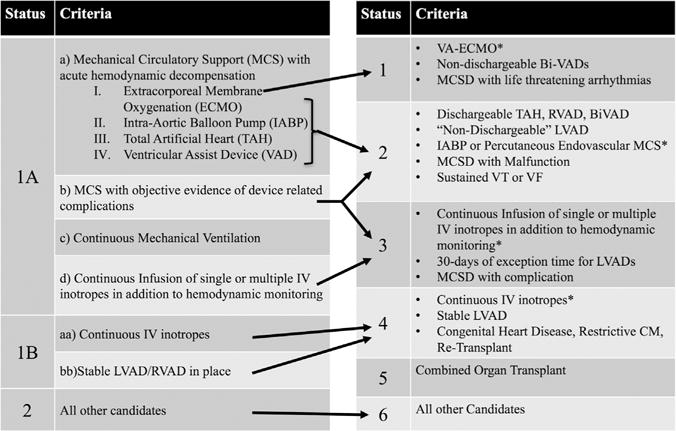
Current and future adult heart allocation. Schematic depiction of the shift from the current adult heart allocation system to the modified system. *Cardiogenic shock requirement applies. (Constructed with permission directly from the policy details in Organ Procurement and Transplantation Network.).
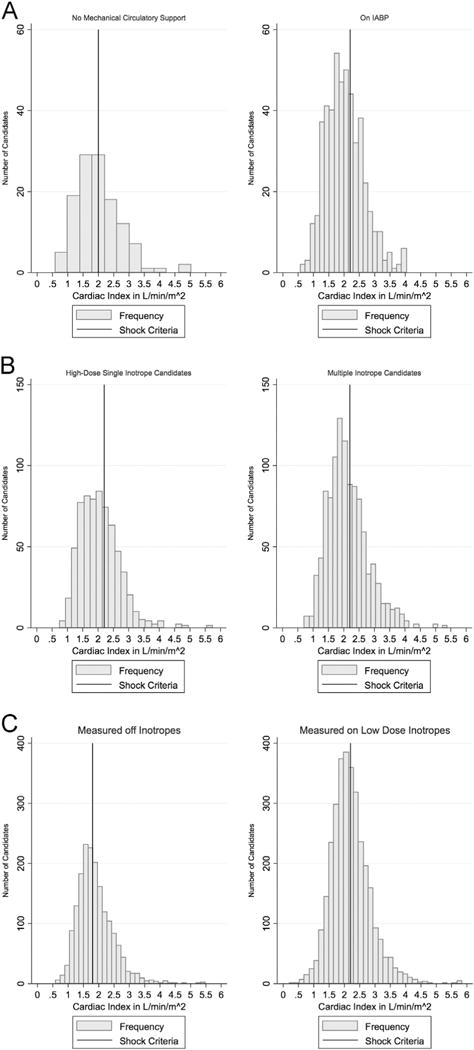
(A) Cardiac index of candidates supported by an IABP at the time of listing. The histogram on the left is of cardiac indices for candidates without circulatory support at the time of hemodynamic measurement. The histogram on the right is of cardiac indices of candidates supported with the listing IABP at the time of hemodynamic measurement. The vertical lines represent the cutoff for cardiogenic shock, 2.0 liters/min/m2 for candidates without mechanical support at the time of listing and 2.2 liters/min/m2 for candidates supported by IABP. Candidates to the right of the line would be ineligible for Status 2 listing. (B) Cardiac index of candidates supported by high-dose single inotropes or multiple inotropes at the time of listing. The cardiogenic shock cardiac index criterion (<2.2 liters/min/m2 when supported by inotropes) is marked with a vertical line. Candidates to the right of the line would be ineligible for Status 3 listing. Candidates supported by multiple inotropes had a higher cardiac index (mean 2.24 liters/min/m2 vs 2.16 liters/min/m2; p = 0.018) and were more likely to be ineligible by shock criteria for Status 3 than candidates supported by high-dose inotropes (74% vs 40%; p< 0.001). (C) Cardiac index of candidates supported by low-dose inotropes at the time of listing. The histogram on the left is of cardiac indices for candidates not on inotropes at the time of hemodynamic measurement. The histogram on the right is of cardiac indices of candidates receiving low-dose inotropes at the time of measurement. Candidates to the right of the line would be ineligible for Status 4 listing. For candidates with hemodynamics measured before inotrope initiation, the mean cardiac index was 1.88 liters/min/m2, and the proportion of candidates disqualified by shock criteria was 49%. For candidates with hemodynamics measured on the listed inotrope, the mean cardiac index was 2.21 liters/min/m2, and the proportion disqualified was 46% (p = 0.027 for shock proportion comparison).
References
-
- Organ Procurement and Transplantation Network. Modify adult heart allocation 2016 2nd round. Available at: https://optn.transplant.hrsa.gov/governance/public-comment/modify-adult-.... Accessed December 15, 2016.
-
- Colvin M, Bolch C, Pyke J, Skeans M, Wang X, Zeglin J. Analysis report: data request from the Heart Subcommittee of the OPTN Thoracic Organ Transplantation Committee. 2015 Oct; Data Request ID: HR2015_01.\.
-
- Singh TP, Almond CS, Taylor DO, Graham DA. Decline in heart transplant wait list mortality in the United States following broader regional sharing of donor hearts. Circ Heart Fail. 2012;5:249–58. - PubMed
-
- Narang N, Thibodeau JT, Levine BD, et al. Inaccuracy of estimated resting oxygen uptake in the clinical setting. Circulation. 2014;129:203–10. - PubMed
-
- Balik M, Pachl J, Hendl J, Martin B, Jan P, Jan H. Effect of the degree of tricuspid regurgitation on cardiac output measurements by thermodilution. Intensive Care Med. 2002;28:1117–21. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
